Public Questions Log
We want to be open and transparent about the way we do business. We want to ensure local people and groups have the opportunity to ask The Shrewsbury & Telford Hospital NHS Trust Board of Directors questions about the Trust’s work. This page contains the questions sent to us by members of the public following Trust Board meetings. For information about submitting a question please visit our Questions to the Trust Board page.
Public Questions Log – 14 December 2023
Question Number |
Meeting Date |
Questioner |
Questions and Answers |
|---|---|---|---|
| 2023/001
Received: 29/12/23 |
Agenda Item: 150.23 & 160.23 | John Crowe | Agenda item 150.23, 2a states – ‘Infection Prevention and Control: cleaning in the Emergency Department – while routine cleaning is still taking place, deep cleans cannot be done due to the intense overcrowding caused by high demand and insufficient flow.’ |
| 2023/001
Received: 29/12/23 |
Agenda Item: 150.23 & 160.23 | John Crowe | 1. Please advise each of the specific features of incapacity SaTH management attribute to be each of the cause/s of A&E ‘intense overcrowding’ ?
The pressures faced in our Emergency Departments, wards and the wider care sector are complex, multi-faceted issues requiring a systemwide response and long-term transformation. The pressures in our emergency departments are related to multiple factors, including significant and sustained demand across the system, outdated configuration and layout of our emergency departments, and increasing numbers of patients with frailty and more complex conditions. This contributes to a longer waiting times, with patients spending more time in our emergency departments, whilst waiting for an inpatient bed to become available. We recognise there are a significant number of patients who no longer need acute care and are waiting to be discharged into community care. This is not the standard of care we would wish to provide and we remain grateful for the ongoing support and patience of patients and our dedicated colleagues as we work in this challenging environment. There are a range of factors that affect patient flow into and out of a hospital, and we are working within the Trust, and with partners, to improve the timely discharges of patients into the community to release much-needed inpatient hospital beds. |
| 2023/001
Received: 29/12/23 |
Agenda Item: 150.23 & 160.23 | John Crowe | 2. Please advise each of which department/s and/or committee/s within SaTH is/are addressing each of the cause/s of A&E overcrowding ?
We know that urgent and emergency care isn’t just an issue for the medicine and emergency care division and across all of our divisions, clinical, operational and corporate colleagues, as well as system partners, are working to ease the pressures faced in our emergency departments and improve care for patients. It requires an integrated, clinically-led approach through long-term transformation. The Trust has adopted the same proven methodology utilised in our maternity transformation work in a dedicated emergency care transformation programme. The focus is within the emergency pathways, however, there is further work ongoing across the Trust to improve ward processes, discharges, and work across our system with partners through the Urgent and Emergency Care programme. The progress of these transformation programmes is reported to our Emergency Care Transformation Assurance Committee, with direct reporting links to our Board and also the system Urgent and Emergency Care Board. |
| 2023/001
Received: 29/12/23 |
Agenda Item: 150.23 & 160.23 | John Crowe | 3. In the interests of patient safety (increase in SaTH A&E deaths noted) please advise a) each of the actions SaTH is i) taking and ii) planning to provide capacities to meet patient need demand, to avert ‘intense overcrowding’ in A&E, to allow deep cleans; b) by which date will each of these be delivered?
There has been a significant amount of work undertaken in the Trust, and working with our system partners, to manage the pressures faced within our emergency departments and hospitals. In addition to our internal transformation programmes, we are working with partners on a range of short-term and long-term initiatives that will support the timely discharge of patients from hospital and alleviate the pressures faced in our emergency departments. This includes the launch of new rehabilitation and recovery units at both RSH and PRH in January, and continuing to increase usage of new community services, including the Outpatient Parenteral Antimicrobial Therapy (OPAT) service and the Virtual Ward team, with the Shropshire Community Health NHS Trust. We are also continuing to work with the ambulance services to minimise unnecessary conveyances to hospital and reduce ambulance handover delays with our Ambulance Receiving Areas and enhanced Same Day Emergency Care services. All of this aims to facilitate flow into and out of our hospitals and ease pressure in our Emergency Departments. Our multi-million pound Electronic Patient Record digital investment will also provide our clinicians with the systems they need to improve flow. The first phase of this three year programme will go live in April 2024 with the introduction of a new Patient Administration System. We are working closely with national NHS experts in hospital discharges and have been open to trialling new ways of working and sharing best practice. Whilst we have made good progress in some areas, including reducing the time taken for initial assessment in our emergency departments, we recognise we have much more to go to transform the way we work across the Trust and with partner organisations. Looking forward, significant progress is also being made with our vital plans to transform our acute hospital services through our Hospitals Transformation Programme (HTP). The HTP Outline Business Case (OBC) has recently received Government approval. The HTP will see the Princess Royal Hospital in Telford specialise in planned care and the Royal Shrewsbury Hospital specialise in emergency care. The plans have been designed, led and supported by clinicians and will improve the quality of care that we deliver for our communities across Shropshire, Telford and Wrekin and mid Wales. We are now preparing our Full Business Case (FBC), which is the final stage in the national approval process. We are committed to continuing to work closely with our local communities, patients, and colleagues every step of this journey. For more information on opportunities to get involved, please contact the Public Participation for further information sath.engagement@nhs.net. In the meantime, we are continuing to maintain cleaning standards in the departments, through:
|
Public Questions Log – 13 October 2022
Question Number |
Meeting Date |
Questioner |
Question |
Answer |
|---|---|---|---|---|
| 2022/000
Received: 12/10/2022 |
Agenda Item: 180.22 IPR | Gill George | Concerns raised about letters being received from patients removing them from the treatment waiting list at their request, when no such request has been made. It was thought this may have affected hundreds of patients and patients are subsequently being informed it is due to a computer error. | For background information, there was an issue with cancellation letters that were being sent to patients whose referrals had been rejected on the Electronic Referral System (ERS) by a Consultant after the doctor had read and assessed the information. Some referrals were then rejected as the patient did not require a hospital appointment.
The letter the patient should have received should have said that the consultant had assessed their referral and decided that they patient either needed advice and guidance from their GP, who the consultant would advise which means that the patient doesn’t have to wait many months for an unnecessary hospital appointment, or that the patient needed to be redirected to the most appropriate Consultant, so the patient gets more quickly to the correct consultant. The patient’s GP would be sent the detail from the consultant as to why the referral has been rejected via ERS so should have been able to advise the patient. So this is not a cancelled appointments issue but an IT issue. Appointments are appropriately not being made for patients after consultant review if the appointment is not clinically required and more appropriate treatment is appropriate. However incorrectly worded letters have been generated for patients which does not make this clear and is causing confusion, which we are trying to remedy. Since we became aware of the problem, we have asked our medical secretaries to double-check any consultant-rejected referrals and advise the appointment booking team so they can generate the correct letter. Last Updated: 21 October 2022 |
| 2022/001
Received: 12/10/2022 |
Agenda Item: 180.22 IPR | Gill George | How many patients have been affected and over what timescale? |
We have contacted our printing outsourcing company who have been able to provide us with information for the last 90 days of patients who have been sent a letter stating that they have declined treatment. This is all that is kept on the print archive. The file contains a total of 1,361 patients who have now been validated as a result we have identified 99 patients who have received an incorrect letter. We will contact the GP Surgery for these patients to ensure that the patient has been contacted and that the advice given by the Consultant has been enacted. |
| 2022/002
Received: 12/10/2022 |
Agenda Item: 180.22 IPR | Gill George | What is the cause of the error? | See above – the error is due to an incorrect letter being sent which does not clarify that a consultant has reviewed the referral letter and identified, and shared with the patient’s GP, a more clinically-effective way of dealing with the presenting issue. |
| 2022/003
Received: 12/10/2022 |
Agenda Item: 180.22 IPR | Gill George | Has it been resolved, and if so when? | A temporary solution has been identified where the medical secretaries advise the appointments team of the decision made by the consultant so the booking team can manually select the correct letter. This process will remain in place whilst an IT solution is sought. |
| 2022/004
Received: 12/10/2022 |
Agenda Item: 180.22 IPR | Gill George | What steps have been taken to identify and contact every individual patient who has been affected, including those who may struggle for whatever reason with written information? | We have asked Synertec (the company who print our letters) to provide data on patients who the “cancelled” letters have been sent to ensure we have identified all patients affected. Currently, we require that all such letters are held back and only sent after validation by our team. This will remain in place until we are sure the issue is resolved. |
| 2022/005
Received: 12/10/2022 |
Agenda Item: 180.22 IPR | Gill George | Is it possible that any patients have slipped through the net? | No patients have slipped through the net. When referrals are rejected or returned to referrer with advice from either a booked appointment or a triage service, the patient’s GP practice is notified through e-Referrals. All practices monitor e-Referrals daily, paying urgent attention to Rejected Responses. |
| 2022/006
Received: 12/10/2022 |
Agenda Item: 180.22 IPR | Gill George | If the Trust is not 100% confident that every patient removed from the treatment lists by error has been contacted and rebooked, is it time to deal with this much more publicly by working with the media and urging patients to come forward? | The key message is that this is an IT error and that patients have not been cancelled but a more appropriate way of managing the patient’s presenting issue has been clinically recommended by the consultant, and the GP advised of the same. If patients have any concerns, they should contact their GP who should be able to update them. |
Public Questions Log – 12 May 2022
Question Number |
Meeting Date |
Questioner |
Question |
Answer |
|---|---|---|---|---|
| 2022/001
Received: 20 May 2022 |
12/05/22
Agenda Item: 082/22 Integrated Performance Report |
Gill George | The report notes that £7.570 m of efficiency savings were achieved in 2021/22. How were these savings achieved, and from which service areas? Were reductions in local audiology clinics part of these efficiency savings, and are there any plans to restore local audiology services? (I gather the Bishop’s Castle audiology service has gone, and that Ludlow patients are currently being advised to attend PRH – a challenging journey by public transport).
Which service areas have been identified to date for recurrent savings in 2022/23? |
Q: The report notes that £7.570 m of efficiency savings were achieved in 2021/22. How were these savings achieved, and from which service areas? Were reductions in local audiology clinics part of these efficiency savings, and are there any plans to restore local audiology services? (I gather the Bishop’s Castle audiology service has gone, and that Ludlow patients are currently being advised to attend PRH – a challenging journey by public transport). Which service areas have been identified to date for recurrent savings in 2022/23?A: The 2021/22 efficiency programme delivered £7.6m of savings, this was split 53% recurrent and 47% non-recurrent. • £3.9m of savings related to a reduction in agency spend across many services due to the recruitment of substantive international nurses • £3.3m related to non-pay schemes with £1.4m of rates rebates, £0.8m of pharmacy efficiencies and • £0.6m relating to procurement.The 2022/23 recurrent savings are planned to be delivered from ongoing international nurse recruitment and non-pay savings from procurement, pharmacy, and divisional schemes.There were no efficiency savings that related to the audiology service.In relation to the audiology service at Bishops Castle, an audiology service has not been provided there for several years due to the clinic rooms not meeting the necessary clinical standards (due to poor acoustics). We do still try to offer care closer to home wherever possible and have audiology appointments available at both Ludlow or Church Stretton for those in the south of the county.Last Updated: 01 June 2022 |
| 2022/002
Received: 20 May 2022 |
12/05/22
Agenda Item: 082/22 Integrated Performance Report |
Gill George | The report notes a staggeringly high (and very concerning) staff turnover of 2.19% in nursing and 2.5% amongst Allied Health Professionals in March 2022. This is attributed to ‘special cause concern’ and therefore recognised as something ‘out of the ordinary’. What causal factors have been identified as lying behind this high percentage of core clinical staff leaving the trust? | Q:The report notes a staggeringly high (and very concerning) staff turnover of 2.19% in nursing and 2.5% amongst Allied Health Professionals in March 2022. This is attributed to ‘special cause concern’ and therefore recognised as something ‘out of the ordinary’. What causal factors have been identified as lying behind this high percentage of core clinical staff leaving the trust?
A: The slight peak of 2.19% in nursing and 2.5% in AHP staff is mainly attributed to a number of colleagues choosing to retire in March. Many individuals choose to retire at the end of the tax year ie in March as there are a number of recognised tax advantages in doing so (new tax year will result in entitlement to full annual personal allowance, lower rate of income tax if a higher tax rate payer and other investment allowance advantages) It should be noted that 50% of leavers in March were attributed to retirements with 35% of those opting for flexi-retirement, meaning these are colleagues who will be returning to the Trust as part of our flexible retirement offer. Since January-22, the Trust has successfully welcomed 26 AHPs and 122 nursing and midwifery colleagues resulting in a higher number of colleagues joining the Trust from both staff groups than those who have chosen to leave. Last updated: 01 June 2022 |
| 2022/003
Received: 20 May 2022 |
12/05/22
Agenda Item: 086/22 Freedom to Speak up Report |
Gill George | The report shows a relatively high percentage of midwives (3.5%) spoke up in Q1 and Q2. This plummeted to 0.35% in Q3 and 0% in Q4. The Ockenden final report was published in Q4. Is it possible that midwives were suddenly much happier, or did midwives feel less confident about speaking up in Q3 and Q4? Why did some maternity staff contact the review team to request that their evidence was removed from the final report, expressing a fear of being identified? Is it correct – as Donna Ockenden reported – that some maternity staff were told by their managers not to speak to the independent review team? |
Q: The report shows a relatively high percentage of midwives (3.5%) spoke up in Q1 and Q2. This plummeted to 0.35% in Q3 and 0% in Q4. The Ockenden final report was published in Q4. Is it possible that midwives were suddenly much happier, or did midwives feel less confident about speaking up in Q3 and Q4?
Why did some maternity staff contact the review team to request that their evidence was removed from the final report, expressing a fear of being identified? Is it correct – as Donna Ockenden reported – that some maternity staff were told by their managers not to speak to the independent review team? A: Since the beginning of 2022 the Division has implemented a number of different and accessible ways for maternity staff to give their views directly so they can be assured they are being listened to, rather than relying just on the Freedom to Speak up route, which is still there and has also been enhanced by access to an external organisation (Protect) who staff can contact should they wish. These additional routes also include fortnightly drop-in sessions and visits to wards and departments by the Senior Leadership Team (including the Executive Team). There is also a new senior leadership team in the Division who have adopted an “open door” approach for all staff. There is also a new online platform called Improvewell, which capture’s staff’s views and the views of staff are fedback through the Maternity Transformation Programme, in which Culture is one of the 7 workstreams. All of these supports are to encourage staff to raise concerns directly and as early as possible, with a commitment from the Chief Executive that all concerns will be listened to and responded to. These many different routes reflect the investment that the Trust has made in enabling concerns to be raised. The Freedom to Speak Up team still visit the Maternity areas directly to ensure face to face that there is no negative consequence from these changes All maternity staff were encouraged and supported by their managers and the Trust to contact and provide information to the Ockenden review team to ensure the Trust gained maximum feedback on services and care. Staff were also made aware through regular Trust communications and briefings of how to contact the review team directly and give their feedback For personal reasons it appears a small number of staff requested for their evidence to be removed from the final Ockenden report. This was their decision and although staff were offered support from the Trust the final decision remained with the individual. It is not correct that managers told maternity staff not to speak to the team. This would have been taken very seriously had it occurred. Last updated: 01 June 2022 |
Public Questions Log – 08 November 2021
Question Number |
Meeting Date |
Questioner |
Question |
Answer |
|---|---|---|---|---|
| 2021/001
Received: 19 November 2021 |
08/11/21 | Gill George | • Is the Board confident that it acts at all times in accordance with the Nolan Principles of Public Life? Could the reply focus on how the current approach to Future Fit/HTP work satisfies the following principles: o Accountability: Holders of public office are accountable to the public for their decisions and actions and must submit themselves to the scrutiny necessary to ensure this. o Openness: Holders of public office should act and take decisions in an open and transparent manner. Information should not be withheld from the public unless there are clear and lawful reasons for so doing. o Leadership: Holders of public office should exhibit these principles in their own behaviour and treat others with respect. They should actively promote and robustly support the principles and challenge poor behaviour wherever it occurs |
We note the use of the updated descriptor for ‘Leadership’[1] which now places more emphasis on treating others with respect and address this accordingly.
The members of the Board of Directors, individually and collectively, are responsible for setting the culture, or the ‘tone’, of the organisation. Over the course of the last 18 months or so in particular, they have applied candour and admitted to their mistakes (and those of others before them, where appropriate) and apologised for the consequences experienced by patients, colleagues, stakeholders, members of the local communities, regulators and partners. This new openness has been demonstrated already and will continue to be the foundation of how we transact business as leaders. The Trust is subject to regulatory processes laid out in the NHS transactions guidance for trusts undertaking transactions, including mergers and acquisitions (2017). (Currently out for consultation until 21 December 2021.) The guidance governs the way in which NHSI/E assures large transactions involving NHS Trusts and uses a standardised transaction framework to assess risk. As funding is being provided from the Department of Health and Social Care, the Trust is also subject to the Capital regime, investment and property business case approval guidance for NHS providers. A link providing all the regulatory guidance documents, appears below, together with details the processes, at each stage, which the Trust needs to pass through, for completion of the transaction: Compliance with the required – lengthy – processes to progress the HTP project, demonstrate the Trust’s accountability for its statutory obligation to “exercise its functions effectively, efficiently and economically.”[2] There may be legitimate reasons why some matters/details cannot or should not be publicised at a particular point in time. One of the principal pieces of legislation to which we sometimes refer is the Freedom of Information Act 2000. In the case of the HTP, it has been stated already by the Trust that detailed plans will be published in the future, subject to agreement with NHSI, a party to the transaction; this may invoke a section 22 exemption from publication at this time. Additionally, a section 43 exemption – commercial interests – may also be appropriate. [1] The Committee on Standards in Public Life (November 2021) Upholding Standards in Public Life: Final report of the Standards Matter 2 Review, pg8 [2] National Health Service Act 2006, sec. 26 Last updated: 08 December 2021 |
| 2021/002
Received: 19 November 2021 |
08/11/21 | Gill George | The written report to the Board comments: “The draft SOC has now been submitted to NHSEI for regional and national approval. When it has been approved, a summary of the content will be made available, in line with national protocols.” In response to a Board member, Chris Preston explained that the public would be provided with the content of the SOC made accessible to them ‘in a simple and easy way’.
When does SaTH anticipate publication of the SOC itself, rather than a version re-written for public consumption? Also, which national protocols are being referenced here, and please can you provide a link to or a copy of them? |
The Trust is intending to publish both a summary and the full draft SOC when the case has progressed through the required regulatory approval processes. We have confirmed with NHSEI that this is in line with the standard approach taken for other similar cases. The timing of publication will be dependent on the time taken to complete the regulatory approval processes.
Annex 3 of the capital regime, investment and property business case approval guidance requires that all approved SOCs for schemes over £50 million are made publicly available by Trusts – please see 1.11 in the NHSEI guidance: https://www.england.nhs.uk/wp-content/uploads/2020/08/NHSI_Capital_Regime_Investment_Annex_3_final_v2.pdf Last updated: 08 December 2021 |
| 2021/003
Received: 19 November 2021 |
08/11/21 | Gill George | In his verbal report, interim Deputy Chief Executive Chris Preston emphasised that the last version of the Strategic Outline Case was completed in 2019 and that since then, the clinical and operational position ‘is quite different’; the financial position is different both as a trust and as a system; care pathways have changed; there is an increased focus on integrated care; and there are changes to regional and national requirements.
Despite changes to the SOC to incorporate all of these things, the ‘outputs of public consultation’ in a very different NHS context and – perhaps – on a very different set of proposals reportedly remain valid. Is this a credible position, when so much has changed at Trust level, in the local system, and within NHS England? Has the Trust taken legal advice on this? |
The Shropshire, Telford & Wrekin Clinical Commissioning Group (CCG) is the responsible statutory body for agreeing and commissioning these service changes. The CCG approved the Decision-making Business Case (DMBC) for the service reconfiguration in 2019. The Trust has been asked to lead the implementation of the proposed service model described in the DMBC, on behalf of the CCG and the Integrated Care System. The draft Strategic Outline Case (SOC) appraises the options to deliver the agreed future service reconfiguration and recommends a preferred way forward. The CCG has reviewed the draft SOC and provided the Trust with a Letter of Support. Last updated: 08 December 2021 |
Public Questions Log – 05 August 2021
Question Number |
Meeting Date |
Questioner |
Question |
Answer |
|---|---|---|---|---|
| 2021/001
Received: 13 August 2021 |
05/08/21 | Gill George | There has been a sharp increase in the number of concerns raised by midwives, a much sharper increase than for any other staff group. (Your report shows an increase from 2 and 3 concerns in Q2 20/21 and Q3 20/21 to 15 in Q4 20/21 and 10 in Q1 20/21).
‘Attitudes and behaviours’ seem to be the prominent issue – but what lies behind these? What is the current vacancy rate for midwives, and how does this compare with a year ago? |
Q1 The number of concerns raised by midwives
The Freedom to Speak Up (FTSU) team have deliberately increased their visibility with all the midwifery teams, including Community midwives, to encourage greater confidence in raising issues so they can be addressed in a timely way. This has included the FTSU team giving presentations on the process and the outcomes and the importance of raising issues and the support that is available to do so. The FTSU team have also held a series of drop-in sessions so midwives can talk to them privately and in more detail about any concerns that they may have, so they feel fully supported to speak up. The increase in numbers of concerns raised by midwives is considered a positive development and ensuring clear feedback to all those who do speak up will hopefully encourage greater confidence in the process, by all staff groups, as the FTSU team go forward. It is recognised that midwives have required additional support following the national interest in maternity services and this will continue to be provided. This focus on midwives has been a deliberate strategy by the Trust and the FTSU team and has also been supported by the Director of Nursing who has personally encouraged midwives to raise concerns and reassured them of the positive support that is available. This also links with our “Courageous Conversation” Masterclasses that have been provided across the Summer as part of the Leadership development programme. Q2 Current vacancy rates and comparisons to one year ago Current vacancy rate – the Trust has just successfully completed a recruitment drive, which will see 17 substantive midwives starting over the coming weeks. Once they are in place the Trust will have 6wte substantive vacancies Substantive vacancies one year ago were 6.7wte. Last updated: 13 September 2021 |
| 2021/002
Received: 13 August 2021 |
05/08/21 | Gill George | Ambulance Waits: Does SaTH review individual cases of harm resulting from very long waits? Are you aware of cases of harm?
Do you expect the additional 32 beds in February 2022 to solve the problem, and, in a directly relevant question, does the intended increase in beds exceed the intended decrease in acute beds in current plans for HTP/Future Fit? |
Q1 Does SaTH review individual cases of harm resulting from very long waits? Are you aware of cases of harm?
At times when the department is very busy and there isn’t the physical capacity or workforce to treat all patient simultaneously (which could be around 80 patients during “surge” periods), like all Emergency Departments we will treat on the basis of clinical priority regardless of where the patient is waiting. The ED team work with the Ambulance crew to clinically review all patients waiting to be offloaded so that we can treat patient based on their clinical need whether they are waiting in an ambulance , cubicle or waiting room. At times of peak activity this is important as we need to be sure we treat the sickest patients first. We work closely with the ambulance crew who will also alert us to any deterioration in the patient’s condition and ensure the patient remains under review while waiting, thus avoiding any harm and we always seek to move patients into the ED building as soon as possible so the crew can be released. If it transpired any harm had occurred we would complete an incident form in the normal way for review by the Patient safety team, but we take all steps to avoid this. Q2 Do you expect the additional 32 beds in February 2022 to solve the problem, and, in a directly relevant question, does the intended increase in beds exceed the intended decrease in acute beds in current plans for HTP/Future Fit? The plans for a 32 bed modular ward at RSH will not solve the overall bed capacity shortfall, but it will go some way to closing it. The Trust continues to work on further capacity options, as a Trust and with our Integrated Care System partners. The capacity will be vital to help cope better with the higher levels of urgent care demand as well as Covid that we are seeing. The Hospital Transformation Programme is currently reviewing future bed requirements as part of the work being undertaken by the Trust to develop an updated Strategic Outline Case (SOC). Our future bed projections will consider the latest demographic and potential non-demographic changes including the expect impact of planned new local care pathways and utilisation of community services. This will determine whether there will be any changes to the original bed requirements as set out in Future Fit. Last Updated: 13 September 2021 |
| 2021/003
Received: 13 August 2021 |
05/08/21 | Gill George | FUTURE PLANS:
Will SaTH share the current HTP assumptions, in the interests of transparency? Will SaTH’s Chair use her influence to lobby for ICS plans to be made public? If not, why not? |
Thank you for your Public Trust Board question(s).
Question 1): Sharing of Assumptions in HTP Plans The Hospital Transformation Programme (HTP) is currently reviewing a range of planning assumptions as part of the work being undertaken by the Trust and ICS to develop and update the Strategic Outline Case (SOC). Once this is complete, the draft SOC will be reviewed by regulators and considered further prior to any approval being given. We will ensure that any changes to planning assumptions are set out in the SOC which is submitted to regulators. Delivering HTP also supports key parts of our wider strategy such as developing new models of care that will transform our services, which are being designed collaboratively with our partners to improve the quality and integration of health and care services. We are now moving through the business planning phase and I am delighted that we have appointed an external supplier, PA Consulting, to support the finalisation of the Strategic Outline Case (SOC) over the coming months. As part of the development of the SOC we will be addressing a number of key challenges:
Timelines are still indicative, but we are aiming to submit the SOC later this year, complete the Outline Business Case by mid-2022, the Full Business Case by mid-2023 and complete construction by mid-2028. Please note these timings are dependent on sign-off by NHSEI. The SOC will be made available to the public once it’s been through the relevant approval processes. Question 2): Future Publication of Integrated Care System (ICS) Plans The SaTH Chair (Deputy ICS Chair) and all other members of the ICS Board confirm that they are committed to publishing all relevant ICS papers / documents, so that the citizens of Shropshire, Telford & Wrekin can engage in plans and monitor progress. This includes the ICS System Development Plan (which is the ICS’ main strategy document and references the Hospital Transformation Plan and supersedes the Long Term Plan), once it has been through relevant approval processes. The personal position of the SaTH Chair regarding publication of relevant documents is fully aligned with the ICS Board’s position. Last updated: 24 August 2021 |
Public Questions Log – 10 June 2021
Question Number |
Meeting Date |
Questioner |
Question |
Answer |
|---|---|---|---|---|
| 2021/001
Received: 18 June 2021 |
10/06/21 | Gail Appleton | Context
On 23 May 2019, The Shrewsbury and Telford NHS Trust received a letter from Baroness Dido Harding which shared the outcomes and recommendations from an NHS Improvement Advisory Group investigation, requesting that the board review and assess the procedures for the management and oversight of local investigation and disciplinary procedures that were in place in May 2019 and assess them against the Advisory Group’s recommendations. In addition, the Trust was asked to review any cases currently being considered to ensure that they demonstrated an inclusive, compassionate and person-centred approach and demonstrated best practice in line with these recommendations. Question i) Were the board made aware of how many suspensions were ongoing at that time and were all of these cases reviewed at board level, as requested by Baroness Harding, in line with item 7 of the guidance. ii) Were impact assessments undertaken with each of these employees to assess how the suspension had affected them? iii) Can the board offer offer reassurance that they have a full understanding of the effect that the disciplinary process had on the individuals who were on suspension at that time and that ‘safeguarding of people’s health and wellbeing was paramount and continually assessed’ in line with item 6 of the guidance. |
Thank you for your Public Trust Board question(s).
We can confirm that The People and OD Team have been working with the Dido Harding recommendations since they were first received in 2019. We continue to also consult with staff, managers and staff representatives on improvements to our policies as part of our ambition to continue to improve the Culture and Leadership at The Trust. We believe practitioner health and well-being support should always form a large part of any process. Examples of this work has been ensuring the Trust Board monitors the progress of all suspensions/exclusions and other significant cases. The Trust Board receive regular updates which describe the work we are continuing to do to improve the experience of our staff. This includes, Health and Wellbeing support, suspensions/exclusions, tribunals, length of cases and significant learning points for the Trust that have been identified through multidisciplinary case reviews. The Trust Board continue to receive regular in-depth reports where progress and actions are agreed and monitored. We continue to engage with all colleagues and partners through our ‘Making a Difference’ platform which since 2020 has provided us with continuous feedback so that we can continue to improve. During 2021/2022 all our Leaders are mandated to undertake Leadership Development to support our ambitions for the People Strategy. Specifically relating to suspensions and exclusions, the Trust has a robust risk assessment that must be completed and approved by an Executive Director in all cases. Regularly reviews take place for any member of staff suspended or excluded; practitioner health and well-being support forms a large part of this review process. In line with Baroness Harding’s recommendations this is discussed with the member of staff at regular reviews to ensure appropriate support and that the full impact of the effect of the suspension on their health and wellbeing is understood. This has been routinely in place since 2019. The Board take the oversight of local investigation and disciplinary procedures very seriously and expect an inclusive and compassionate approach to staff during these difficult processes. Last updated: 02 July 2021 |
| 2021/002
Received: 18 June 2021 |
10/06/21 | Gill George | Context
The Operational Summary report covers 12 hour breaches, and ‘flow’ through ED and into wards being a challenge. The RCEM view is that ‘exit block’ from EDs typically reflects bed availability. Question
|
Thank you for your Public Trust Board question(s).
The average core number of Adult General and Adult Acute inpatient beds at SaTH is currently 670. Comparatively, in 2020/2021 there were 649 and in 2019/2020 there were 637. However, the actual number of beds in use can vary dependent on various factors. When inpatient demand is greater than inpatient bed capacity, escalation beds can be temporarily opened within areas such as day units providing additional bed capacity, facilitating additional flexibility for the trust to cope with fluctuations in demand. Conversely, the number of beds available can be reduced if it has been deemed necessary, for patient safety purposes, to instigate infection prevention and control restrictions temporarily reducing the use of inpatient ward areas during infectious outbreaks. The current HTP modelling indicates an increase of circa 50 general and adult inpatient beds by 2026. The analysis is currently being updated to incorporate latest demographic and case-mix information along with the expected impact of new local care pathways and utilisation of community services. Last updated: 02 July 2021 |
| 2021/003
Received: 18 June 2021 |
10/06/21 | Gill George | Context
The Director of Nursing reported concerns over skill mix: that the percentage of Registered Nurses in the nursing team was 55% at SaTH against a minimum 65% in national guidance. Question 1) Is the one-on-one replacement of 120 Registered Nurse posts with Nurse Associates an ongoing SaTH objective and part of HTP Policy? 2) how has the percentage of Registered Nurses in the nursing workforce changed in recent years; and is SaTH now committed to driving up that percentage? |
Thank you for your Public Trust Board question(s).
1) Is the one-on-one replacement of 120 Registered Nurse posts with Nurse Associates an ongoing SaTH objective and part of HTP Policy? There is no plan to replace 120 Registered Nursing posts with Nursing Associates, either now or as part of HTP. Nursing Associates play a valuable role working alongside Registered Nurses (RNs) and HealthCare Assistants (HCAs) as part of the clinical team. The role of Nursing Associate was introduced nationally in 2017 to bridge the gap between HCAs and RNs and also offer a career opportunities for HCAs who wish to progress through their career in nursing to a graduate-level role. Nursing Associates will provide support to the clinical teams and work alongside RNs and other members of clinical team but not replace them. Guidance and resources to help support the integration of NAs and shape workforce plans will be issued by the national team later this year and SaTH will play an active role in enriching our nursing workforce to improve the quality of patient care and service delivery. We hope this will improve staff retention through career progression and provide opportunities to enable us to “grow our own” nursing workforce. We are also planning to offer a “top up” course for those NAs who wish to progress to an RN. SaTH also has a number of other recruitment and retention strategies which include;
2) How has the percentage of Registered Nurses in the nursing workforce changed in recent years; and is SaTH now committed to driving up that percentage? There has been a steady increase in RNs over the last 12 months, despite all the challenges of a global pandemic, which has seen the skill-mix increase from 50% in 2020 to 55% in January 2021, our bi annual staffing reports identify the improvements made and the Trust is supportive of increasing the skill-mix percentages in line with the National picture. We are working very closely with colleagues in Workforce and Health Education England to achieve this and to recognise the special challenges that a rural organisation faces. One of our strategic goals is that “our staff are highly skilled, motivated, engaged and live our values”. SaTH launched a new preceptorship research project in September 2020 supported by our Research Matron and the National Institute for Health Research – we are working towards achieving the Capital Nurse Charter Mark and plan to move to a 12-month rolling preceptorship programme from January 2022, whereby all new recruits to the Trust will have an opportunity to access preceptorship whenever they join. We have an extensive programme of health and wellbeing to ensure all staff feel supported which offers psychological, physical, emotional and financial support to all our staff. We also offer great careers with opportunities at all levels with favourable terms and conditions including generous annual leave entitlement and pension provision, fair, inclusive and family-friendly policies supportive of work-life balance, flexibility and job security. We also recruited international nurses, all of whom passed their Objective Structured Clinical Examination (OSCE) to join the Trust. We also offer a “Golden ticket” scheme whereby instead of a formal interview, student nurses from Staffordshire University attend Values-based conversations throughout their training, with a final conversation at the start if their third year. If they obtain the required qualifications and reflect the Trust values they will be offered a “golden ticket” to a position at SaTH when they qualify Last updated: 22 June 2021 |
| 2021/004
Received: 18 June 2021 |
10/06/21 | Joy Stocks | It has always been standard practice for SaTH to publish its Operating Plan for the year. When will you share with the public the Operating Plan for 2021/22? If this is a system Operating Plan, will you – via the ICS Vice Chair – support the publication of the system plan? | Thank you for your Public Trust Board question(s).
The Integrated Operating Plan is based on guidance issued NHS England and NHS Improvement (national bodies in charge of the NHS). It is standard practice each year for this guidance to be published early in the calendar year to allow planning to take place ahead of each new financial year. Due to temporary changes made to this system as a result of the national response to Coronavirus the Trust, like all other Trusts, is currently operating with operating guidance that covers only the first half of the financial year. However, the Trust is planning for the full year and has prepared a draft integrated operating plan which has been shared with the Trust Board in private. This integrated plan (referred to in the Board papers) is the internal SaTH plan and it is the intention of the Trust to share the integrated operating plan at a future Board meeting in public once we are assured that the full requirements for the year are known and we have planned appropriately. Any system operating plan would be published directly by the Integrated Care System and we would of course ensure that we aligned with that. Last updated: 28 June 2021 |
| 2021/005
Received: 18 June 2021 |
10/06/21 | Joy Stocks | The chart on Bed Occupancy (page 32) suggests there are between 600 and 650 G&A beds available, excluding ‘restricted beds’. Is this correct? How many additional restricted beds exist (and are they still restricted because of Covid-19)? | Thank you for your Public Trust Board question(s).
I can confirm this relates to 51 beds in our base of 670 adult beds which were restricted/ring-fenced for certain categories of patients to ensure beds were available. At the time of this chart in April these were; 12 for urgent elective activity at RSH 17 for renal patients 22 for oncology patients At this time the number of Covid patients was low and continued to reduce. Last updated: 28 June 2021 |
| 2021/006
Received: 18 June 2021 |
10/06/21 | Joy Stocks | The Finance and Performance Assurance Committee report comments on the move of Renal Dialysis away from PRH. Why will Renal Dialysis be moved, where will it be moved to, and what public consultation has taken place? | Thank you for your Public Trust Board question(s).
Currently no decision has be made regarding this potential service change, however we have had several meetings with our communities and patients to discuss the potential move. If the service change was to go ahead the service would continue to be provided by SaTH staff, providing dialysis treatment in a spacious, fit for purpose unit that has the capacity to provide additional dialysis stations. The dialysis unit would be within the community rather than a hospital setting, however its location is still near to the Princess Royal Hospital. Please see details of our engagement so far below:
Patients and the public who could not attend any of the above meetings were also provided with contact details to ask question or provide feedback. For your information I have attached the presentation given to patients and the public about this potential service change. The Trust has committed to have further patient and public involvement should the Trust progress further with this potential service change. Last updated: 22 June 2021 |
Public Questions Log – 08 April 2021
Question Number |
Meeting Date |
Questioner |
Question |
Answer |
|---|---|---|---|---|
| 001/2020 | 28/05/20 | Gill George | Relating to the period 1st January 2020 to the present: How many cancer patients have had their treatment delayed during this period? Who took decisions on this? What criteria were in place to determine who would be treated and who would not? I understand a decision was also taken to withhold diagnostic information from some patients (i.e. they were not told of a newly diagnosed cancer). Their treatment was therefore also delayed. How many patients were affected? Again, who took decisions on this, and based on what criteria? Were the Medical Director, Chief Executive and Board aware of the decisions to delay diagnostic information and treatment to some cancer patients? |
An extract from the minutes of the Board of Directors’ meeting on 28/05/20. At the beginning of the pandemic (March 2020) there was a clear national steer to cancel as many inpatient, ambulatory appointments and procedures as possible, in order to protect vulnerable people and create the capacity to deal with any potential surge due to the pandemic.
Whilst SaTH maintained a number of urgent surgical procedures and a full programme of radiotherapy and chemotherapy, in responding to the pandemic, the Trust recognised there have been a number of cancer patients whose diagnostics and treatment have been delayed. The Trust is not aware of any patients where the outcome of their cancer diagnosis was deliberately withheld. If you have evidence of such information being withheld, the Trust would ask you to forward it to David Holden, Interim Director of Governance (David.holden7@nhs.net). It will be investigated and the appropriate action taken. |
| 002/2020 | 30/07/202 | Gill George | The April 2020 report (from a 2019 inspection) is quite damning. It shows a failure to improve in very many areas, and a deterioration in some.
The ‘well led’ domain continues to be rated as inadequate. The report notes that the Trust breached its CQC registration with regard to 11 regulations. These included ‘Regulation 5: Fit and Proper Persons- directors’; ‘Regulation: 17: Good Governance’ and ‘Regulation 20: Duty of Candour’. These areas are fundamental. Without strong and principled leadership, the Trust will of course struggle to provide high quality clinical care. Major weaknesses in leadership were identified by the CQC in November 2018. Many of those concerns evidently remained a year later. What were the ‘Fit and Proper Persons’ breaches in November 2018? What steps were taken to resolve these? What were the ‘Fit and Proper Persons’ breaches a year later, in November 2019? Do these breaches still exist? A lack of understanding of Duty of Candour has caused great distress in the past, not least in the Trust’s handling of avoidable deaths and harm in the maternity service. What is the evidence that the current leadership team has meaningful commitment to the Duty of Candour, including a willingness to fight for a culture of openness and transparency across the organisation? Does the current Board recognise there have been damaging failures around candour in the recent past? Public board meetings since November 2018 have failed to identify ongoing weaknesses around leadership. Why? Has the Board been unaware? Or did the Board choose to withhold concerns around leadership from the public? Is the Board confident that leaders with the skills to achieve fundamental transformation at SaTH are now in place? Assuming the answer is ‘Yes’, what is the basis for that confidence? |
At the time referred to, effective governance systems were not in place to ensure all director files were complied with the ‘fit and proper persons’ regulation. The Trust could not therefore be assured that all directors were ‘fit and proper’ to carry out their responsibility for the quality and safety of care.
The Trust has since improved governance including the review of the Fit and Proper policy. The Trust commissioned its newly appointed auditors to ensure systems and processes are up to speed and good practice is being followed and maintained. |
| 003/2020 | 30/07/20 | Gill George | Former Chief Executive
What external support has SaTH received from Virginia Mason in the last year? Has this included any input from former SaTH Chief Executive Simon Wright? |
Simon Wright has not had any input into SaTH through his Virginia Mason work. |
| 004/2020 | 30/07/20 | Gill George | Staff Survey
The 2019 staff survey showed particular weaknesses around ‘themes’ of Health and Wellbeing and Staff Engagement. What steps is the Board taking to ensure that staff feel valued, listened to and supported through a difficult period? Will the Trust seek to ensure the involvement of all staff in current and future service changes, encouraging staff to see themselves as the champions of patient care and safety, and placing staff at the heart of change? The history has perhaps been one of over-reliance on a small group of senior medical staff. |
The Trust has recognised and now focused on the issues that impact staff. These include ensuring staff feel valued, listened to and supported.
The health and wellbeing of the staff re- mains a critical priority – and never more so than during this Covid period. Actions taken include:
The Trust recognises there is more to be done and we will continue to identify staff needs and respond to them. With a new leadership team in place, the Trust has already taken steps to put staff alongside patients at the heart of service changes. As an example, the Hospital Transformation Programme has been consulting with staff groups and clinical teams across the organisation about the future configuration of services. This will continue throughout the autumn to ensure their views are fully reflected in the Outline Business Case. Staff at all levels are being consulted, including Facilities, Estates, Administration and other support services, not simply senior medical and nursing staff. A new monthly information Cascade designed to reach all staff, has been well received which includes an opportunity for staff to give feedback and ask questions which are channelled back to the senior team. |
| 005/2020 | 30/07/20 | Gill George | Maternity Dashboard
The report of the Maternity Assurance Committee notes ‘A maternity dashboard was presented to the meeting’. The maternity dashboard used to be published and in the public domain as a matter of course. It was withdrawn by SaTH at a time of mounting concern about the maternity service. I have asked for publication of the maternity dashboard to be reinstated at least twice in the past. Maternity is an area of significant public interest, and it is in the interests of transparency for SaTH to share this information. Will SaTH publish the current maternity dashboard? Will SaTH make this maternity dashboard, along with previous and future maternity dashboards, available on its website? |
The Maternity Dashboard has been un- der review for several months and re- mains under review to ensure it meets national standards and follows good practice. The Trust will be reviewing publication of the dashboard, the context of the data and the Statistical Process (SPC) charts. |
| 006/2020 | 30/07/20 | Gill George | Births Before Arrival (BBAs); MLUs
(This data will be recorded by SaTH as a matter of routine and should take a few minutes to look up). |
BBA data is not a direct reflection on closure of the MLUs. This would only be significant if the number of BBAs were specifically Midwifery led women, as it is these women who should be booked for care and birth at an MLU. |
| 007/2020 | 30/07/2020 | Gill George | Cancer follow up care
This question is asked at the request of K, a SaTH patient: I’m 35, with young children. I have a serious gynaecological cancer. My initial treatment of major surgery was successful, but I continue to need regular review appts because the consequences of recurrence could be very serious indeed. My SaTH consultant has stressed the critical importance of these reviews and of these happening on time. My last booked review would have been 8 weeks overdue – but it was then cancelled, with one day’s notice. I had to make a fuss to get another appointment arranged, earlier this month. My consultant highlighted again – not just to me but to the wider service – the importance of scheduled follow up happening on time. I am due for a vault smear in early October. I received a letter from SaTH seeking to replace my appointment for a smear with a telephone appointment! This is meaningless. Again, I have had to take the responsibility for sorting out my own care. I’m tired and unwell. Cancer has changed my life. I don’t want to have to take on the job of arranging my own care, and I think many others in my situation would be unable to do this. What’s happening? Has your system for offering follow up to cancer patients broken down in the last few months? Why? What steps will SaTH take to audit existing cancer patients to ensure that people who have not been offered appropriate care will now receive high priority appointments? |
During Covid-19, cancer services continued as a priority. All appointments were triaged by a consultant to ensure that an appropriate appointment option was offered. Where appropriate, telephone follow ups were offered rather than face to face, and some follow up appointments were converted into telephone or consultations via other means.
It would not be usual for a smear appointment to be replaced with a telephone call, but this may have been a result of consultant triage as above. Waiting time targets continue to be achieved in gynaecology, and all patients on a follow up list are reviewed. |
| 008/2020 | 30/07/2020 | Claire Howard, Parkinsons UK | Parkinson’s Nurse Specialist (PNS) post
In December 2019, following a number of conversations and meetings over the previous eighteen months, SaTH’s Chief Operating Officer and Assistant Chief Operating Officer informed Parkinson’s UK that the Trust had committed to recruiting to the vacant Parkinson’s Nurse Specialist (PNS) post. However this post is still vacant and has not been advertised. Parkinson’s UK understands the constrictions Covid placed on trusts’ capacity for recruitment but we are also keenly aware that, for more than two years, people with Parkinson’s have had limited access to a specialist nurse service in Shropshire. We are also aware that a number of other trusts have success- fully recruited to these posts in recent months. Please can the board advise when the post will be advertised?” If there are any problems with this then please let me know. 29/07/20 It’s great to hear that there is a plan to recruit and would be grateful to be kept updated on this process. I would also just like to confirm that this question will still be presented to and answered by the board this afternoon so that there is public acknowledgement of this? I hope that this would also then provide some reassurance to the Parkinson’s community in Shropshire. |
SaTH has a Parkinson’s Specialist Nurse in post based at PRH in Neurology Services and is in the process of recruiting a second one. |
| 009/2020 | 30/07/2020 | Diane Peacock*
* This question following the July 2020 Board meeting was one of a number raised at the Community Engagement meeting in December 2021 and it was agreed that the original response had not addressed the question so these were re-considered by a number of senior staff, including
Click here Community Engagement Meetings – SaTH to see response issued December 2021 which reflected the position at that time, which was some 18 months after the original meeting. |
Various Questions
The questions below are intended to provide the public with information relating to the local outcomes of national directives and guidance on hospital admissions and discharges, from and into care homes in Shropshire and in Telford & Wrekin during Covid-19. In the interest of accessibility and transparency, the Governing Body is politely requested to supply actual numbers and dates when responding to questions 1-5.
|
|
| 010/2020 | 30/07/20 | David Sandbach | Various Questions
Replacement wording ‘Prof Deadman (NED) high- lighted that the same serious WLI implementation policy issues appear to have been identified and reportedly resolved by successive audit committee re- views in the last 9 years. We therefore need to check that when WLI audit actions are reported as completed they result in lasting improvements. Yet another example of bad management at SaTH this comment looks like others whereby NED’s complain about management inability to make plans stick on a permanent basis. See also – “Mr Allen (A.NED) made the point with regard to action plans that the Trust is good at finding solutions but these are not sustainable.” What does “embedded” mean?
“the Trust’s Maternity Assurance Committee is also adding performance assurance rigour into the Care Group” In February this year I pointed out this facility:
Source: MBRACE Perinatal Mortality Surveillance Report page 38. Given the real time nature of this reporting system I would expect the Executive led Maternity Quality Committee and the MAC would find it a very rigorous assurance measurement tool. “Prof Deadman (NED) stated that he was pleased to note that the Trust has implemented an outpatient virtual consultation solution as part of the response to Covid-19.” SEE: https://www.sath.nhs.uk/patients-visitors/video-clinics/ Why have some of the surgical specialties e.g. vascular and colorectal not signed up to offering virtual clinics? Has an evaluation methodology / evaluation team been established? “Mr Newman asked if the Trust has a date by which it will be back on plan for cancer performance and diagnostics. He noted that the IPR is reporting the historical position, and provides no evidence of service recovery proposals. The COO responded that as part of the immediate restoration work the Trust has introduced some urgent services, and that extensive discussion is currently underway on how restoration is further developed as part of the Operational Plan.” May 28th 2020 Board members may like to see this report from the SCCG Board papers dated 8th July 2020 to get a feel for the situation in the Shropshire CCG area:
https://www.shropshireccg.nhs.uk/media/2818/08072020-combined-part-1-sccg-governing-body-papers.pdf MONTHLY INTEGRATED PERFORMANCE REPORT The Board of Directors noted the report, and the Chair requested that future reports incorporate a more forward looking focus. Need to check this is in the Board papers. “The committee received a high level Draft Maternity Transformation Plan to bring the maternity services to where we need to be in the future. This is largely based on themes identified from the leaked DO re- port and aligns to Morecombe Bay report.” Should the people of Shropshire, especially women of childbearing age, raise a glass of campaign to whoever leaked the DO report? Emergency Department Assurance Committee Key Issues Report The fundamental risk to Emergency Department performance is the mad cap, NHS establishment denial of reality by the SaTH Board, CCG’s and NHSE/I. (Recovery Plan included on agenda for discussion at Finance & Performance (August 2020). Unless and until there is a centralised A&E department along the lines of the FF plan SaTH performance will remain abysmal for the next 5 – 6 years. These words will appear in the audit reports year on year: “KPMG was not satisfied that the Trust made proper arrangements to secure economy, efficiency and effectiveness in its use of resources. This was due to its financial position, high agency spend, inadequate CQC rating, failure to deliver a number of operational targets and the independent review into maternity care.” I truly wish the SaTH Board did not believe that the earth is flat and that fundamental forces of clinical demand spread over two half-baked departments cannot be managed by re-arranging the corporate policy furniture and so called “help” from people who do not have any real skin in this game. The backlog of patients waiting for Diagnostics and Treatment has risen significantly during Q1 and additional capacity will be required to address this during the remainder of 2020/21”. No Board paper explaining what the plan is to deal with the issue. A winter pressure plan is promised for the Board in September a few weeks before winter starts in the NHS. “We are planning carefully for the months ahead including winter.” CEO report NEDs need more detail – as do the public. This comment is not good enough at this point in the winter planning cycle: I refer you to my plan to open a Covid safe facility in Telford – at least it is a plan. NEDs should open these links and ask if SaTH has plans to introduce this technology “Call before you Attend service.” https://www.england.nhs.uk/wp-content/uploads/2020/07/Agenda-item-5-Future-of-UEC-services.pdf and this https://www.theguardian.com/society/2019/may/23/birmingham-to-begin-accident-and- emergency-online-chat-service-in-tech-revolution-for-nhs-care SATH UTC Activity and care at the MIUs continues to provide patients with a beneficial alternative to ED” This is not what the SCCG is saying in their Board papers.
Is this performance because SaTH is short of MRI’s and CT scanners? |
The Trust has reviewed these audits and found no evidence of fraud. The Trust has reviewed job plans with individual consultants and identified explanations for audit findings relating to job planning and flexible working. It has provided clearer guidance for doctors. The Trust has amended relevant policies and introduced improved more accountable processes.
In the CQC improvement plan, embedded means, sufficient time has been allowed to ensure systems, process and change have occurred to ensure the action is completed. For example: Following the development of a new pol- icy, embedding would mean actions are applied consistently with tangible and measurable benefits for patient out- comes. Cancer forecast included in Operational Plan (slide 5 & 6). Detail included in August IPR will be presented at Board of Directors Meeting on 17.09.20. Recovery Plan included on agenda for discussion at Finance & Performance (August 2020). The Trust is exploring the “Think 111 first” model and has requested data from other Trusts using it. Recognising the availability of other options, the Trust is being mindful not to increase ED attendances and is working with partners to expand the urgent treatment centre models. The activity taking place at MIUs continues to allow some patients to access care at the 2 MIU sites rather than attend the 2 Emergency departments – this reduces risk for staff and patients. The graph (attached) relates to the national diagnostic standard (DM01) – the aim is for 99% of planned diagnostic tests to take place within 6 weeks of the referral. The standard includes not only CT/MRI/Ultrasound, but also Endoscopy and Physiological Measurements such as ECGs and Audiology. In May, in line with national guidance, routine diagnostics were paused. SaTH was, and still is, unable to carry out the same number of tests per hour as pre-Covid. Referrals to all diagnostic modalities are prioritised based on clinical urgency. Pre Covid, SATH had one of the highest usage rates per scanner for CT and MRI in the region, and reductions in throughput due to social distancing and infection control measures does mean that the Trust requires more scanner capacity. In July, August and September, NHSI have supported SATH with mobile CT, and in October we will have both mobile CT and mobile MRI capacity to support increased imaging. |
| 011/2020 | 08/10/2020 | Diane Peacock*
This question following the July 2020 Board meeting was one of a number raised at the Community Engagement meeting in December 2021 and it was agreed that the original response had not addressed the question so these were re-considered by a number of senior staff, including
Click here Community Engagement Meetings – SaTH to see response issued December 2021 which reflected the position at that time, which was some 18 months after the original meeting |
How can it be acceptable that the SaTH information system is not able to ‘derive’ data on the numbers of hospital inpatient deaths that relate to care home residents based in Shropshire and in Telford & Wrekin (STW)? | Currently the Trust does not have systems in place to produce this information. The local CCG has also confirmed, that currently they also do not have systems in place to produce this information. The CEO advised it would be appropriate to the Trust to be able to provide this information in the future and this will be worked on for the future. |
| 012/2020 | 08/10/2020 | Diane Peacock*
* This question following the July 2020 Board meeting was one of a number raised at the Community Engagement meeting in December 2021 and it was agreed that the original response had not addressed the question so these were re-considered by a number of senior staff, including
Click here Community Engagement Meetings – SaTH to see response issued December 2021 which reflected the position at that time, which was some 18 months after the original meeting |
Can the Board please assure the public that written questions and Trust responses for July 2020 will be published retrospectively and, in future public questions with Trust responses are reported in full? | Response’s have been published previously.
The Trust welcomes questions from the public, as they offer a different perspective on the issues discussed and additional insights into the challenges patients, staff and communities face. The Trust requires questions to be sub- mitted 48 hours prior to the public meeting, so the Board of Directors have time to prepare the answers. This is important as many questions require some research. The Trust will aim to answer as many questions on the day of the Board meeting as possible. Those for which an immediate response could not be prepared will be acknowledged on the day. The Trust will post the answer to outstanding questions on the website by the next meeting (or sooner where possible). If the Trust is unable to post a response within this window, the question will be acknowledged on the website, with a timeline for response. |
| 013/2020 | 08/10/2020 | Diane Peacock*
This question following the July 2020 Board meeting was one of a number raised at the Community Engagement meeting in December 2021 and it was agreed that the original response had not addressed the question so these were re-considered by a number of senior staff, including
Click here Community Engagement Meetings – SaTH to see response issued December 2021 which reflected the position at that time, which was some 18 months after the original meeting |
The fact that outbreaks affecting care home residents in STW have been relatively low compared to other areas means local intelligence on possible causal factors could be exceptionally informative when planning to safeguard local care home residents in the event of a future surge. Given the claim that a system-wide, multi-agency partnership approach was adopted locally to deal with the first Covid-19 outbreak, why is it that a multi-agency evidence base – to evaluate locally specific multifactorial elements impacting on care home residents – is apparently not available for public scrutiny? | Local health and social care have been integrated in the safe management of patients being discharged to all care set- tings (including domestic homes) during Covid-19. An integrated discharge team and hub manned by hospital, social care and community staff, has been put in place, providing an invaluable function.
Local Authorities, as regional lead agencies, supported by the CCG, commission care homes and the Shropshire Partners in Care (SPIC) coordinate activities across the sector. Unfortunately the Trust does not have access to care home plans and activity. Whilst the Trust continues to monitor patients discharged to a community health and social care setting, it does not have access to the detailed Local Authorities’ lessons learnt from the first wave of Covid-19, and benefits to residents and staff. |
| 014/2020 | 08/10/2020 | Diane Peacock*
This question following the July 2020 Board meeting was one of a number raised at the Community Engagement meeting in December 2021 and it was agreed that the original response had not addressed the question so these were re-considered by a number of senior staff, including
Click here Community Engagement Meetings – SaTH to see response issued December 2021 which reflected the position at that time, which was some 18 months after the original meeting |
The Trust is claiming they are unable to differentiate between those patients discharged to their own home or to a residential care home at the beginning of the Covid-19 outbreak. Why is this information not available either via Capacity Tracker or as part of the various multi agency teams overseeing these pro- cesses? | The Trust’s information systems will not enable an answer to this question and the integrated discharge team hub does not hold this information either. The Trust’s new information system, tentatively scheduled to be installed in the Autumn of 2021 will solve this problem. |
| 015/2020 | 08/10/2020 | Dulcie Howell | Have the Hip Operations at Telford Hospital resumed yet? | This surgical area has been prioritised although some operations have not commenced as quickly as the Trust would like. The Trust’s surgical team has been asked to investigate the individual case and a clinician will be asked to contact Ms Howell |
| 016/2020 | 07/12/2020 | Diane Peacock*
*This question following the July 2020 Board meeting was one of a number raised at the Community Engagement meeting in December 2021 and it was agreed that the original response had not addressed the question so these were re-considered by a number of senior staff, including
Click here Community Engagement Meetings – SaTH to see response issued December 2021 which reflected the position at that time, which was some 18 months after the original meeting |
With regard to the July Board questions relating to data, the response was that the ‘SaTH Information system is not able to derive this data’.
|
|
| 017/2020 | 07/12/2020 | Gill George | Asbestos Management
On 1st August 2019, Chair Ben Reid ordered an independent QC-led inquiry into the circumstances around the unfair dismissal of whistle blower Les Small and the successful 2019 HSE prosecution of SaTH for unsafe management of asbestos on the Shrewsbury site. Did the inquiry ever conclude? Or even begin? If it was abandoned, who took the decision and why? If it reached interim or final findings, will SaTH now publish these? If not, why not? The history of the review is here Maternity Questions around the maternity dashboard and around birthing locations were asked of the July 2020 Board meeting but were not answered. They remain relevant, and I request that the questions below are picked up. (SaTH’s maternity dashboard disappeared from the public domain as the scale of its maternity crisis became increasingly clear. This has been queried on several occasions, and assurances have been given that this will be published as a routine part of Board papers going forward. Sadly, this has not happened.) Maternity Dashboard The report of the Maternity Assurance Committee notes ‘A maternity dashboard was presented to the meeting’. The maternity dashboard used to be published and in the public domain as a matter of course. It was withdrawn by SaTH at a time of mounting concern about the maternity service. I have asked for publication of the maternity dashboard to be reinstated at least twice in the past. Maternity is an area of significant public interest, and it is in the interests of transparency for SaTH to share this information. Will SaTH publish the current maternity dashboard? Will SaTH make this maternity dashboard, along with previous and future maternity dashboards, available on its website? Numbers: Births Before Arrival (BBAs); MLUs; CLU How many BBAs have taken place so far in 2020/21? How many BBAs took place in 2019/20? How many BBAs took place in 2018/19? How many births have taken place so far in MLUs in 2020/21? How many births took place in MLUs in 2019/20? How many births took place in MLUs in 2018/19? How many births took place in MLUs in 2017/18? (This data will be recorded by SaTH as a matter of routine and should take a few minutes to look up). Additionally, how many home births took place for the years listed above, and how many births took place in the Consultant-Led Unit at PRH (broken down by year for both)? In its response to the first Ockenden report, will the Board reflect on the need for women to have choice and control during pregnancy and labour (emphasised in Better Births as important components of safe care)? And when is Shrewsbury MLU scheduled to re- open? What are the reasons behind the current pro- longed closure of Shrewsbury MLU? (It closed – for the second time – in June 2019 for an estimated maximum period of 6 months). The rural MLUs were closed to maintain staffing levels at the PRH Consultant-Led Unit, with indefinite closure taking place without consultation in June 2018 following repeated short-term and short-notice closures throughout 2017. When is the legally necessary public consultation likely to take place? Future Fit/ Hospital Transformation Programme This immensely troubled and unpopular programme has been limping along since November 2013 now. In the autumn of 2015, the original ‘whole system’ approach was abandoned when NHS England deemed it unaffordable, and it was replaced with an acute-focused programme. Public consultation on this took place over the summer of 2018, at a time when the capital cost of Future Fit was estimated at £312m. Subsequently, Future Fit has been rebranded as the Hospital Transformation Programme. The estimated capital cost of Future Fit has slid about: rising to £498m in a report leaked in December 2019, re- ported to local MPs by SaTH to have risen to £580m in January 2020 (when the then SaTH Chair Ben Reid also described the project as ‘botched’), but the cost was then said by STP Chair Sir Neil McKay as £533m in July 2020. Any information available to the public has been via leaks. The level of secrecy around the project is unprecedented. What is the current estimated capital cost of implementing Future Fit/ Hospital Transformation Programme? If this is unknown, what is the range of capital costs under consideration? What level of capital funding has been authorised to date by NHS England and/or the Treasury? Is this still £312m? Is there an agreed (or even likely) funding source now identified? Can the Trust Board guarantee that the OBC now under development – reportedly via a £6m ‘draw down’ – will include every major component – at both sites – that went to public consultation in the summer of 2018? Can the Trust Board guarantee that any funding shortfall will not result in a phased implementation of the Future Fit/ Hospital Transformation Programme? If the Trust cannot guarantee these things, will you share with the public – the people you serve – the fullest possible information on which elements of Future Fit may be dropped entirely and which may be delayed, and by how long? Local people are the most important stakeholders you have. |
The independent report by Fiona Scolding QC was concluded and presented at the Board of Director’s meeting in Public in July 2020 (Item 2020/099) – Chair’s Report incl. Investigation into the com- plaints made to the Care Quality Commission reported on this matter.
Maternity – response’s published previously. Maternity Dashboard – response’s published previously. As stated at ORAC 25/3 we are commit- ted to supporting women to make choices about their care in pregnancy, labour and birth. We have introduced personalised care plans in order to facilitate this. In Oct 2020 we introduced a monthly MDT meeting to discuss requests for care that falls outside of national guidance in order to mitigate as many risks as possible and to be sure that we have provided the woman with all available information and options. It is also an opportunity to identify any opportunities for training. In December 2019, the definition for Born Before Arrival (BBA) for the Maternity Services Dashboard was changed. Prior to the change, a birth was considered a BBA where the Place of Birth was selected as ‘In Transit’ or ‘Other’. This was changed to the new criteria where the field “Name of Non Professional Person Delivering” contained a name. This was irrespective of the given Place of Birth. The change was due to the number of babies born with Place of Birth given as “Home” and delivered by a Non-Professional. The figures on the dashboard were back- dated to the beginning of the 2019/20 Financial Year. The Dashboard figures per FY for BBAs are:
There is no national data on BBA’s to enable a comparison. NMPA and GIRFT do not include this metric. |
| 001/2021 | 07/01/2021 | David Sandbach | How do you rate your performance in respect of the objectives noted below:
“We want to be open and transparent about the way we do business. We want to ensure local people and groups have the opportunity to ask questions about our work.” Source: https://www.sath.nhs.uk/about-us/trust-infor- mation/questions/ |
The Board of Directors acknowledge that there have been occasions when the Trust could have been more transparent or open about the way it transacts its business. However, there are many opportunities for local people and groups to engage with the Trust by asking questions about the Trust’s work. We have criteria for what will constitute a ‘public question’ on the website.
The Trust’s website provides several links to various ways in which local people can engage with the Trust or with local groups and institutions where stakeholders have the opportunity to ask questions or raise issues In December 2020 attendees at Community Engagement Group meeting, met staff from the Trust, including the Director of Nursing. The Trust currently has circa 10,000 public / patient ‘members’ who engage with the organisation. The Trust’s website provides contact details for patients to provide feedback, raise a concern or complaint, or simply share a story or comment. The website includes examples of how that feedback has improved patient experience at the Trust. The Trust’s website includes details of a Publication Scheme, directing stakeholders to various pieces of information, such as responses provided to those who have asked for information under the Freedom of Information Act 2000. The Trust regularly publishes Trust documents, including the Annual Report and Accounts, the Quality Report, and reports from external agencies and third parties, all Trust expenditure over £25,000, a log of organisations that the Trust shares data with, declarations of interest from senior col- leagues, registers, policies, and more. |
| 002/2021 | 07/01/2021 | David Sandbach | Why is the Integrated Performance Report being hidden from the public? | It had been decided by the Trust that the agenda for the meeting held on 7 January 2021 would, under the circum- stances, focus on the Trust’s response to the Ockenden Report published on 10 December 2020.
For this reason it was agreed that the IPR report would be published on the website as an information pack. |
| 003/2021 | 07/01/2021 | Gill George | Have you had any questions from families?
Also, no one has discussed HOW this happened. How COULD this happen, not just briefly but for decades? And if you don’t know, how can you stop it happening again? I would of course welcome a reply to my letter to the Chair and Non-Executive Directors (attached again here in case it has been mislaid). Finally, the answers to my July questions – only recently discovered – indicate a change of methodology in the collection of data on ‘Births Before Arrival’ (BBAs). This seems to have the effect of approximately quadrupling the number of BBAs, which is a little bit surprising. Could you explain both the old and new methodologies? Does the change in methodology preclude a year by year comparison? If so, how does SaTH monitor its performance in this rather crucial area? If a comparison has been done, I would welcome this being shared. |
Any details concerning correspondence between families affected by the events covered in Donna Ockenden’s First Report, would remain confidential between the Trust and those involved. Hence the Trust is unable to respond to this question.
The letter addressed to the Chair and Non-Executive Directors was responded to on 13th January 2021. In December 2019, the definition for Born Before Arrival (BBA) for the Maternity Services Dashboard was changed. Prior to the change, a birth was considered a BBA where the Place of Birth was selected as ‘In Transit’ or ‘Other’. This was changed to the new criteria where the field “Name of Non Professional Person Delivering” contained a name. This was irrespective of the given Place of Birth. The reason behind the change was due to the number of babies born with Place of Birth given as “Home”– but were delivered by a Non Professional. When making this alteration to the Dash- board, the figures were backdated to the beginning of the 2019/20 Financial Year. The Dashboard figures per FY for BBAs are; o FY2017/18 = 3 o FY2018/19 = 8 o FY2019/20 = 41 (altered criteria active from 01/04/2019) o FY2020/21 = 52 There does not appear to be any national data on BBA’s to enable a comparison to be made – NMPA and GIRFT do not include this as a metric. |
| 004/2021 | 11/02/2021 | David Sandbach | Hospital Transformation Plan.
What does the term “reset” refer to? When will the Board be in a position to publish the Statement of Case supporting the Hospital Transformation Plan? Can you please confirm the model of hospital service provided by SaTH, as per the consultation document and subsequent decisions to have RSH as the emergency hospital and PRH as the planned & diagnostic remain as per the consultation document? £ 6,000,000 has been agreed in principle by NHSE/I to support the initial phase of the HTP planning pro- cess. Has this money been released to the Trust? Maternity There are circa six committees which have some oversight responsibilities for Maternity service. This looks like a complex command, control, coordination and communications system. Is any individual on all of these committees as a mechanism for continuity of input and detailed understanding of what is going on and integrity of the whole process? There appears to be two dates for the implementation of BadgerNet March 2021 and October 2021 when will BadgerNet be implemented? Would the Maternity plan be enhanced and more comprehensive if it had details of the IT facilities needed to support it were made explicit in the plan. Does the SaTH Board expect their EMBBRACE data to improve as a result of the actions being taken post feedback in the Ockenden report? |
The term ‘reset’ relates to updating for- ward plans and milestones, incorporating required actions to improve programme delivery performance and ensuring full alignment with the ICS long term plans.
Timelines for approval (and publication) of the SOC will be determined as part of the programme reset. The model of hospital service remains as per the consultation document. The funds have not been released to the Trust. Hayley Flavell DoN is the Responsible Executive and Chair of Maternity Quality Oversight Committee (MQOC), the extraordinary oversight committee reporting to QSAC, which Ms Flavell attends. BadgerNet implementation was originally set for May 2021, however, it is now pro- posed to implement the system from March 2021. October 2021 refers to the proposed EPR implementation date. The implementation of BadgerNet Maternity and Neonatal EPR is the system required to support the delivery of the plan. The service continues to implement and monitor the impact of national initiatives designed to reduce the rate of avoidable stillbirth and neonatal deaths. There was a reduction in extended perinatal death rate (EPDR) in 2018. And whilst the Trust has continued to observe a downward trend in the crude EPDR it does not have comparative unit data to enable comparison in line with MBRRACE. |
| 005/2021 | 11/02/2021 | Dag Saunders | Is the Trust satisfied with the accuracy level of the lateral flow test for staff? | Lateral Flow Tests (LFT) are an additional tool for identifying a small cohort of asymptomatic staff. They have a high specificity (over 95%) with few false-positive results. Covid-19 tests cannot be 100% accurate.
https://www.ox.ac.uk/news/2020-11-11- oxford-university-and-phe-confirm-lateral- flow-tests-show-high-specificity-and-are# |
| 006/2021 | 11/03/2021 | Linda Senior | Questions around maternity
|
The Shropshire Telford and Wrekin Maternity Voices Partnership is independent to the Trust, but includes colleagues working for the Trust to support its aim to improve maternity care across the region. Individuals (independent women and their families) are able to get involved with the MVP on a voluntary basis – contact details appear on the MVP website – but the Trust has no responsibility to ensure that the MVP is representative of local communities.
The Board has stated at meetings in pub- lic that the decision to suspend the MLU birthing service was on safety grounds due to staffing and the safest use of the available workforce; that suspension will continue until the CCG Review is complete. Safety issues remain paramount. The Board considered the findings from the engagement exercise but the safety of the services was and remains the key priority. July 2018 https://www.sath.nhs.uk/wp-content/up- loads/2018/07/13-MLU-Update.pdf October 2018 https://www.sath.nhs.uk/wp-content/up- loads/2018/10/Maternity-PPT-engage- ment-responses-Sept-18.pdf November 2018 https://www.sath.nhs.uk/wp-content/up- loads/2018/11/09-MLU-Update-Nov- 2018.pdf November 2018 https://www.sath.nhs.uk/wp-content/up- loads/2019/02/02-Minutes-of-29-Novem- ber-2018-Trust-Board.pdf At this stage, the Trust is unable to con- firm or deny whether members of staff have been referred to either the GMC or NMC over the last decade. |
| 007/2021 | 11/03/2021 | Gill George | Future Fit/ HTP
We know that a draft Strategic Outline Case for Future Fit/ Hospital Transformation Programme was submitted to NHS England in November 2019. Will SaTH make this publicly available, and also share the NHS England response? |
This was a draft document that was sub- mitted for comment but not approved, so we are not planning to share it in the public domain – at the time, my understanding is that no formal feedback was received from NHSEI. |
| 008/2021 | 11/03/2021 | Sue Campbell | Future Fit/Hospital Transformation Programme
|
There is a lot of work still to do in this area – and this is one of the key components that we need to focus our collective efforts towards as we move forward, working closely with our health and social care system partners. |
| 009/2021 | 11/03/2021 | Marylin Gaunt | Birth-rate Plus
Culture and Behaviours
Infection Control
Recent press reports have highlighted something slightly different: the discharge home of patients who are Covid-positive who have then infected other fam- ily members. In one case, a relative was casually ad- vised at the point of discharge, ‘Oh by the way, he’s Covid-positive’ (i.e. this was known to SaTH in advance of discharge). What steps is SaTH taking to deal with both problems? Is it considered acceptable practice to dis- charge Covid-positive patients to destinations where the chance of them infecting others is high? |
The Birthrate Plus staffing review to be presented to the Board in June 2021.
The Trust’s ‘new values’ were published in 2020, and are: Partnering, Ambitious, Caring, Trusted, providing the acronym PACT. An outbreak is two cases or more cases. Each case is classified through a robust process including NHSEI/CCG/PHE, chaired by DIPC with assurance provided via IPAC and reported to the Trust Board Board. We were unable to provide a response at the March board meeting, as results were, as noted, published on the same day as the board meeting. However, a much fuller report was presented to the Board at its April meeting, and appears on the Trust website. |
| 010/2021 | 11/03/2021 | David Sandbach | A 95.3% performance would give a very different graph. Is the figure of 95.3% correct? Graph link
NB According to this graph just over 50% of majors are stuck in A&E for longer than four hours. The quality implications of this are very serious. Use of MBBRACE data. Can you please explain your position as stated at last month’s meeting with your current position noted in the new Quality Improvement Strategy: Question from last month: Does the SaTH Board expect their EMBBRACE data to improve as a result of the actions being taken post feedback in the Ockenden report? Answer: “The service continues to implement and monitor the impact of many national initiatives which will lead to a reduction in the rates of avoidable stillbirth and neonatal deaths. The 2018report showed a reduction in extended perinatal death rate (EPDR) and we have observed a continued downward trend in the crude EPDR but the service does not have comparative unit data to enable definitive comparison with MBRRACE.” Quality Improvement Strategy: 05.1 BoD PUBLIC Quality Improvement Strategy incl. COVERSHEET a (sath.nhs.uk) “How will we know if we have succeeded? Reduction in the number of stillbirths, neonatal deaths and maternal deaths measured by MBRRACE FACT MBRACE puts comparative data into the public do- main e.g. size of units by type and numbers of births etc.; also there is a Perinatal Review Tool available. If you have not already done so please fill this form in and you will reap benefits from a quality assurance point of view – PMRT registration form Jan 2018.pdf (ox.ac.uk) Did the meeting close at 16.00 hrs? I attended all of this meeting and seem to remember that it went on until past 17.00 hrs. Why has the SaTH Board not managed to hire a substantive Finance Director? A) Why has the Board not hired a substantive HR Director? Asking someone to act up over long period of time is wrong from an ethical point of view i.e. it looks like exploitation of a loyal employee. Culture – culture don’t you know. Given the frustration with poor progress concerning the Future Fit / Hospital Transformation Programme, which has recently expressed by three of our be- loved local MPs, is the SaTH Board willing to put the Readiness Assessment report into the public do- main. MPs ask health boss for Future Fit plan review | Shropshire Star MP calls for investigation into Future Fit delays | MP asks parliamentary watchdog to investigate Fu- ture Fit delays | Shropshire Star Also is the SaTH Board prepared to make a full and clear statement as to the cause of the hold up on this very vital project? It is well known God ( and the tax paying public) loves repentant sinners. Would it be possible for the SaTH Board to numerate and explain the known milestones referred to above? (picture) How will we know if we have succeeded? Increase in staff and patients recommending ser- vices as a place to receive care including through Friends and Family scores and National Inpatient, Emergency Department, CYP Surveys” Will the SaTH Board publish this kind of data in future? SaTH response rate Feb 2020 NB Data submission and publication for the Friends and Family Test (FFT) restarted for acute and com- munity providers from December 2020, following the pause during the response to COVID-19. The first three months of data will be published in April 2021. For full details see FFT frequently asked questions or email england.friendsandfamilytest@nhs.net See also: Dementia assessment How many out-patient episodes have been provided using the Attend Anywhere facility SaTH has invested in? |
The data in the IPR dashboard is correct – shows 4 hour (67.5%) and split of 4 hour into majors (45.6%) and minors (95.3%). In the exception report the overall 4 hours and narrative is correct – 67.5%.
This graph however is ‘majors’ , whereas the table is ‘minors’ performance –so both correct but shouldn’t have been next to each other. The scheduled closing time of the meetings is 4pm. The meeting last month overran. Our Director of Finance Designate at- tended her first board meeting on 11 March 2021. She will take up the substantive role as from 1 April 2021. This is an internal management document containing some sensitive and commercial information, so we are not planning to share the full report in the public domain at this time. In terms of AttendAnywhere 7230 from mid-April 2020 to end February 2021, since Sept average 235 per week – graph here (which includes Audiology which isn’t in SUS data) |
| 011/2021 | 08/04/2021 | Andrew Metcalf | I have recently discovered that the response of SATH staff to a nationwide survey of NHS trusts rates SATH management literally at the bottom of NHS trusts on such issues as the ease and encouragement of staff to raise concerns about any aspect of clinical or administrative and those same staff’s confidence that they will be listened to, and that is- sues raised will be rigorously investigated and appropriate actions taken by management to improve identified problems.
This is unquestionably a key indicator of significant problems within the managerial culture of SATH compared with other NHS trusts, who are them- selves not highly rated on such questions compared with other industries. There can be little doubt in the mind of any unbiased, open-minded observers or analysts that this major managerial cultural problem is a significant contributor to SATHS widely reported and catastrophic management failings over many years, particularly in maternity care – with little or no evidence of SATH management, acknowledging these problems, taking them seriously or improving their appalling record. I believe that a question from the public highlighting this problem has been tabled for inclusion on the up- coming SATH Board Agenda. In my mind, and based on my discussions with other people served by SATH, addressing this continuing clear and significant management failings, explicitly, urgently and openly, should be right at the top of SATH management’s agenda. This letter, copied to the Shropshire Star, is a formal request to you to ensure that this question of critical importance is included on the agenda for the upcoming SATH Board Meeting. |
It is assumed by the Trust that the question referred to appears below at log numbers 2021/012 and 2021/013
The April board meeting provided an overview of the results of the staff survey and details of some of the work that is ongoing to support staff, the role of culture in creating high quality of care and the work being undertaken in this regard, and details of the ‘Clever Together’ initiative. |
| 012/2021 | 08/04/2021 | Gemma Offand/Jean Macdonald/Joy Stocks/Julia Evans/ Kath Perry/Kayleigh Griffiths/Laura Fletcher/Linda Senior/Penny Dunachie/Rhiannon Davies/Sophie Dick/ Steve Dunachie/Sue Overton/Walt Zak/ William Edmondson/Marilyn Gaunt/Lizzie Fletcher/David Fletcher | Please take this question at your Board meeting on 8th April. I know that most questions from the public are currently being ‘lost’.
The 2020 Staff Survey results for SaTH are truly terrible. One that stands out is that your own staff give SaTH the worst rating of any acute trust in the country on ‘Safety Culture’ – that cluster of questions around staff being able to report unsafe care and the organisation acting to put things right. Patients have a right to know about the safety of their care – but these major safety concerns were not reported to your Board on 11th March and are well hidden in the written report to the 8th April Board meeting. A culture of dishonesty and concealment contributed to the scandal of avoidable deaths in your maternity service. Have you learned the lessons? On 8th April, will your Board make a necessary collective commitment to honesty and accountability to the public you serve? |
Public questions arising from Board Meetings are not ignored, and responses are provided where possible.
The April board meeting provided an overview of the results of the staff survey and details of some of the work that is ongoing to support staff, the role of culture in creating high quality of care and the work being undertaken in this regard, and details of the ‘Clever Together’ initiative. |
| 013/2021 | 08/04/2021 | David Sandbach | At the last SaTH Board meeting it was announced to the WORLD (and all the malicious hackers therein) that SaTH cyber security was wanting.
“Ms Milanec confirmed that implementation of the actions on the plan for the Toolkit, continued, but that lack of oversight in the area of information governance and cyber security had, for some years, been minimal and that the Trust was now having to ‘catch up’.” What action has been taken to inform SaTH partners i.e. the NHS ICS members and THE Local Authorities who are members of the ICS? NB “not being able to demonstrate compliance with the toolkit was potentially problematic.” Catastrophic more like – who wants to hang-out with the weakest link in the ICS? The Board ignores data on compliments. This is a really dumb thing to do because it is not conducive to improving esprit de corps and staff wellbeing. I would like to suggest that the Wellbeing Guardian supports the introduction of direct patient feedback in the form of a web based feedback system. The endorsement / compliment can be fed directly to individual members of staff. How many items are on the risk register? By the looks of things there seem to be at least 2065. Can members of the public have access to the SaTH Risk Register? NB SaTH has a duty of transparency and candid behaviour. “In response the Trust undertook an immediate and complete review of all patients to ensure that appro- priate actions/assessments were in place or com- pleted and that the patients were safeguarded from any potential harm and that mitigations to risks were actioned. These actions were undertaken and com- pleted in response to this condition on the 1st. March 2021.” Will these actions be “embedded” permanently in the SaTH SOP? “but following this overnight stay the child/young person must be transferred to an alternative care setting to meet their mental health care needs if they are not well enough to be discharged.” Is there any evidence the SaTH Board will receive in due course? “The registered provider must adopt an effective system to enable them to identify where all patients un- der 18 are located within the hospital. Appropriate oversight of the care of these patients must be provided by suitably competent staff. This must include continuous oversight by a registered mental health nurse and regular oversight from a child and adolescent psychiatrist for patients under 18 who are admit- ted with acute mental health needs, learning disabilities and behaviours that challenge.” Has this happened and has this caused any placement problems? “Ongoing system wide work is required to further develop responsive, timely, robust quality specialist mental health services to the Trust and address cur- rent gaps in service provision, for example the lack of acute psychiatric liaison services at PRH site be- tween 1am and 8am, and the lack of a Child and Adolescent Mental Health Consultant out of hours to support the Trust. Mental Health services are com- missioned by the CCG and provided to the Trust from MPFT so the system will be working to ensure these are in place moving forward.” Bearing in mind SaTH only has access to one MH Matron is the SaTH Board content that it has enough resources to comply with this condition? Did the SaTH management ever raise the issues regarding service gaps with the CCGs or with the sub- contractor i.e. MPFT. Has the MPFT demonstrated to SaTH management a sincere and unequivocal determination to resolve the problems noted by the CQC? Ditto the new Shropshire & T&W CCG and ICS committee? Bearing in mind the much publicised poor performance in respect of SaTH Maternity Services and the recent CQC report about MH services for children and young people, do the SaTH Board have a corporate bias against youngsters and are youngsters i.e. people 0 – 18 years low priority at SaTH? Does SaTH have a Director of Workforce? The Acting Director of Workforce has been attending SaTH Board meetings since Mrs V Rankin stopped attending SaTH Board meetings in October 2019. 17 going on 18 months is a very long time to have a person in an acting position. When does the SaTH Board expect to employ a substantive Director of Workforce? When will the SaTH Board be in a position to make public the SOC and OBC relating to the Hospital Transformation Plan? “The overall programme is progressing well against the plan. The MoU has now been received for £9.3m in 2021/22 for the RSH ED reconfiguration and the approval process is in motion. This should allow the enabling and main works to start as planned. A firm completion date will be agreed when the contract award process is completed in March 2021.” What plan, when was this plan discussed at the Board meeting? MoU (Memorandum of Understanding) from which organisation e.g. CCG / ICS / NHSE/I / private finan- ciers has SaTH received the MoU? Can members of the public have copies of the MoU document? What is meant by the term ‘reconfiguration’ – is this some reference to building work which is temporary i.e. money which will be spent on propping up the existing A&E at RSH until the Future Fit / HTP building work is complete and SaTH acquires a state of the art ED facility as promised to the public in the FF consultation . In which publication and when was the contract ad- vertised and has it been signed yet? What disruption to patients (i.e. emergency, out patients and in patients) and visitors will the enabling and main works cause and for how long? Why has this project not been mentioned and FULLY explained during an earlier Board meeting? Are the words honesty, transparency, candour and openness embedded (deeply rooted) in the culture of the SaTH Trust Board or like many other things on the Boards last agenda is the embedded bit just too hard for the Board to achieve? |
Ms Milanec further clarified her response, with additional comments, at the April meeting, also confirming that all members of the Board of Directors (save one) had now completed independent Cyber Security Training aimed specifically at Boards.
The Trust does indeed, receive compliments concerning the care that it provides. It has recognised that such compliments should be more publicised, and ways in which to do so, are currently being explored. A response to this question was provided at the April board meeting – circa 500 risks appear on the Trust’s risk register. A summary of the high level risk register will be published on a quarterly basis from May 2021. There is a robust risk assessment. Cascaded across the appropriate areas. Mentally unwell, i.e. not physical – we cannot admit isolated mental health patients. There will be compliance monitoring. System KPI Action plan is tracked via groups that feed into QSAC and board A SOP is in place for oversight Joint working with MPFT re oversight Nurses and medic/ Placement Challenges have occurred both in ED and wards once medically. Escalation in place. A system wide response is required. Additional Mental Health Matron will be joining the Trust in May 2021 focusing on C&YP. This role has been funded by NHSE/I. SaTH management did raise the issues regarding service gaps with the CCGs and/or with the sub-contractor i.e. MPFT. The Trust Board of Directors do not have a corporate bias against children and young people. The Trust has an Acting Director of Workforce. The Trust will employ a substantive Director of Workforce in due course. |
| 014/2021 | 08/04/2021 | Diane Peacock*
* This question following the July 2020 Board meeting was one of a number raised at the Community Engagement meeting in December 2021 and it was agreed that the original response had not addressed the question so these were re-considered by a number of senior staff, including
Click here Community Engagement Meetings – SaTH to see response issued December 2021 which reflected the position at that time, which was some 18 months after the original meeting |
The questions below were submitted to the Board for the December 2020 meeting and remain unanswered and unpublished. Diane Peacock 5.4.21.
With regard to the July Board questions relating to data, the response was that the ‘SaTH Information system is not able to derive this data’. While welcoming the new CEO’s determination in that detailed data be available in future, does the CEO think it was acceptable that basic data on the admissions, discharges and deaths in hospital relating to care home residents could not be ‘derived’ when much of it was in fact available within national repositories such as the NHSE,1 the ONS2 and via local intelligence. The CO-CIN3 reports for SAGE suggest that nosocomial transmission of Covid-19 in the sample started to rise again in October. Has the Trust collated data on cases of Covid-19 occurring up to 14 days after admission to hospital? If so what do the figures indicate, over time, about infection control? In response to an October question about multi- agency working, the Trust stated that: ‘Whilst the Trust continues to monitor patients dis- charged to a community health and social care setting, it does not have access to the detailed Local Authorities’ lessons learnt from the first wave of Covid-19, and benefits to residents and staff’. How can a local authority be expected to learn les- sons from the first wave of Covid-19 unless local intelligence provided by all active agencies is pooled? Does the CEO consider that the pooling of local intelligence including patterns of hospital admissions, discharges and inpatient deaths, relating for example to care home residents, at the height of the pandemic could have helped reduced further loss of life in the second wave to Covid-19? With regard to CQC’s inspection concerns (14.08.20), what is the evidence (qualitative and quantitative) to suggest that all aspects of end of life care at RSH are now meeting the standards all patients deserve? Example: COVID-19 Hospital Activity Example: Weekly provisional figures on deaths occurring and registered in England and Wales by Local Authority that includes of deaths designated to care home/ elsewhere/ home/hospice/ hospital/and other communal establishment 3Example: CO-CIN report |
Response’s published previously. |
| 015/2021 | 08/04/2021 | Gill George | Future Fit/ HTP
What is the estimated cost now of Future Fit/ HTP? Has the expenditure been authorised by the Treasury? How much of this capital has been secured, and from what sources? What is the likely revenue impact annually of the capital required for Future Fit/ HTP? What is the current implementation plan for Future Fit/ HTP (i.e. in what order will stages be implemented and what are your estimated or target dates both for beginning and ending these stages)? We know that a draft Strategic Outline Case for Future Fit/ Hospital Transformation Programme was submitted to NHS England in November 2019. Will SaTH make this publicly available, and also share the NHS England response? “Please take this question at your Board meeting on 8th April. I know that most questions from the public are currently being ‘lost’. The 2020 Staff Survey results for SaTH are truly terrible. One that stands out is that your own staff give SaTH the worst rating of any acute trust in the country on ‘Safety Culture’ – that cluster of questions around staff being able to report unsafe care and the organisation acting to put things right. Patients have a right to know about the safety of their care – but these major safety concerns were not reported to your Board on 11th March and are well hidden in the written report to the 8th April Board meeting. A culture of dishonesty and concealment contributed to the scandal of avoidable deaths in your maternity service. Have you learned the lessons? On 8th April, will your Board make a necessary collective commitment to honesty and accountability to the public you serve?” The opening two paragraphs simply provide the context for our questions to the Board. To avoid any possibility of confusion, the questions to the Board are these: Importantly, will you now respond to the public questions previously submitted to you in 2021? Will you also update the ‘Public Questions Log’ – frozen in time at 7th January 2021 – to show all submitted questions, enabling the public to keep track of which questions are answered and which questions are ignored. Is the Board familiar with the NHS constitution, and its commitment that ‘The NHS is accountable to the public, communities and patients that it serves’? Is the Board familiar with the Nolan Principles of Public Life? These include accountability, openness and honesty. Has the Board had recent training in the Principles of Public Life? Will the Trust Chair circulate the NHS Constitution and Nolan Principles to every Board member? Will she commit to reminding all Board members of the importance of the Principles of Public Life at the start of every Board meeting, public and private A like? The Ockenden report has been revealing. Does the Board agree with us that a greater degree of accountability, openness and honesty from predecessor SaTH Boards might well have saved lives? Has the Board discussed if, arising from events in maternity, there are lessons to be learned around its own culture and way of working? In Future Fit (or its current Hospital Transformation Programme brand name), SaTH is implementing the greatest changes in local health care that have taken place for many decades. You and the CCG together are doing this in near-total secrecy. Inevitably this suggests you have something to hide. In the interests of accountability, openness and honesty, will you now publish the fullest possible information on Future Fit, including your current plans, the proposed timetable for implementation, and the best information available to you on funding arrangements (including capital cost, the likely source of this capital funding, and its potential revenue impact)? A comment in passing, but the Covid pandemic has stretched the local NHS to its limits. If SaTH had successfully implemented Future Fit in 2015, you would have had many fewer beds and nurses available to you over the last year. If public opposition had not stopped the 2016/17 Shropshire CCG assault on community hospitals, there would have been many fewer community beds too, and little or no chance of moving urgent care to Bridgnorth. And a related question: how has Future Fit/ Transformation Programme modelling been updated to reflect the experiences of the Covid pandemic and the likely impact of ‘long Covid’ on population health? What maternity issues or concerns have been identified through the current involvement of Sherwood Forest NHS Trust? What measures have been recommended by Sherwood Forest, and what steps have been taken by SaTH in response? Will you ensure that public Board papers will, as a matter of course, include the appendices made available to Board members? |
The cost for this reconfiguration at pre- consultation business case (PCBC) stage in 2016 was £312m. In the revised 2019 draft SOC, the funding requirements had increased to £533m, predominantly due to increases in published government inflation rates and changes to technical classifications (which in total add £162 million to the predicted capital cost).
Many of the variables will continue to change as we progress through the programme and updated estimates of the capital cost will be summarised as the scheme moves through the business case approval cycle. Other capital schemes of this nature nationally, where development is taking place over a number of years, are also being impacted in similar ways. The projected increase in costs would have applied to all of the options that were considered prior to consultation. In March 2018, the Department of Health and Social Care approved £312 million of funding. The sources of funding are being re- viewed as part of the finalisation of the SOC. The annual capital charges (based on the latest capital costs) are estimated to in- crease by circa £30m (based on the estimates included in the 2019 draft SOC). However, in taking forward the scheme the Trust expects to generate significant annual revenue savings that will be used to offset. We fully expect the programme to deliver the service changes outlined in the public consultation. System partners and stakeholders, including people impacted by the reconfiguration such as patients, families and the wider population of the health system will be kept informed and involved as the programme progresses. The Trust uses an internationally recognised organisation to undertake demand and capacity modelling for the HTP. The demand and capacity models allow for regular adjustment to reflect the most up- to-date circumstances. An updated version of the demand and capacity model- ling will be included in the finalised SOC. There is a lot of further development required in this area and this is one of the key components that we need to focus our collective efforts towards, working closely with our health and social care system partners. Linked to the recommendations of that review, a number of key focus areas were identified and are being progressed at pace:
The delivery of the timelines for the finalisation of the SOC and the development of the OBC are also dependent upon the timely release of the required funding from NHSE/I. The Trust recently undertook a review of the HTP to assess current status and re- set future plans (as the impact of the COVID-19 pandemic reduces). the capital charge increase. Since the last board meeting, a review of questions received from the public over the last few months, has been reviewed. Where questions are able to be answered factually, they have been. All questions are considered, none are ignored. The April board meeting provided an overview of the results of the staff survey and details of some of the work that is ongoing to support staff, the role of culture in creating high quality of care and the work being undertaken in this regard, and details of the ‘Clever Together’ initiative. Yes, the board is familiar with the NHS Constitution, and the more recently refreshed Handbook to the NHS Constitution. Yes, the board is familiar with the Nolan Principles of Public Life. Each board member, as part of their induction, receives a copy of the Principles, and NHS Constitution, together with other information. See above See above May public board agenda, item 101/21 provides an update on the HTP. Further information will be published when it is available. The Board is aware of inaccurate media reports of maternity concerns having ‘been identified’ by Sherwood Forest Hospitals NHS Foundation Trust. No measures were recommended or actions taken. Opinion sought Opinion sought The Board is aware of an inaccurate media report which suggested that concerns had been raised by Sherwood Forest NHS Foundation Trust. No recommendations were made, or steps taken. Yes. |
| 016/2021 | 08/04/2021 | Linda Senior | One of SaTH’s ‘Immediate and Essential Actions’ arising from the Ockenden Review is ‘listening to women and families’. A central strand of achieving this is working with the Maternity Voices Partnership (MVP).
Does the Board have assurance that the MVP is representative? For example, does it include women/families who have lost a baby or who have had a baby harmed in SaTH’s care? Or who have been harmed themselves? Does it include rural women who have been directly affected by the continued closure of rural MLUs? If not, how will you ensure these voices are heard? What is SaTH’s legal justification for the continued closure of the three rural MLUs? Please explain in particular how you have adhered to Section 242 of the NHS Act 2006 (the Duty to Involve). A pretence that the closures are temporary is not compelling four years on. How did SaTH take into account the outcome of pub- lic engagement on MLU closure that took place in the summer of 2018? (This showed very strong community support for community MLUs to re-open). The paper on SaTH’s response to the Ockenden Review includes many, many actions that are ‘on track’, but not yet delivered. The ‘not yet delivered’ actions include many strands around safety and risk assessment, listening to women and ensuring informed consent, consultant/specialist involvement in complex cases, adherence to national guidelines etc. These are core components of safe maternity care. What does this tell the Board about the maternity service that has existed until a few months ago and perhaps continues to exist? What does this tell the Board as a whole about its own lack of oversight and its failure over many years to challenge both its Executive and its clinical leaders within Maternity and Women’s and Children’s? There is strong reason to believe that ‘attitudinal’ problems contributed very substantially to avoidable deaths and harm in maternity over a period of decades. In particular, there seems to have been an ative failure to learn from very senior members of staff in Maternity and Women’s and Children’s. Is the Board entirely comfortable that senior staff members continue to hold influential positions within SaTH and continue to shape the future of patient care (and patient safety) delivered by the Trust? How many staff members have been referred to the GMC as a result of patient safety issues in the maternity service over the last decade? And how many have been referred to the NMC (for the same rea- son, and the same period)? |
Response’s published previously. |

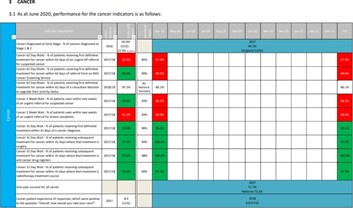
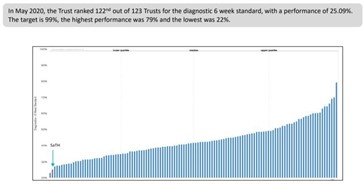
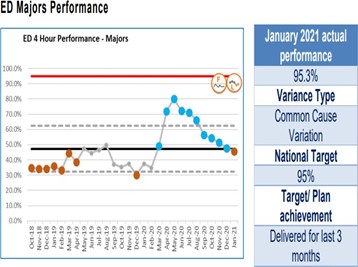{kind=link}
{kind=link}
{kind=link}
{kind=link}
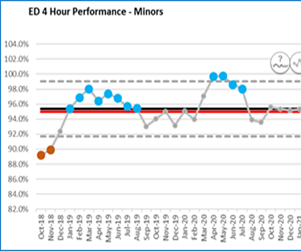{kind=link}
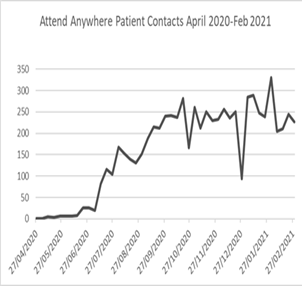{kind=link}
Public Questions Log – 07 January 2021
Question Number |
Meeting Date |
Questioner |
Question |
Answer |
|---|---|---|---|---|
| 2021/01 | 07/01/2021 | David Sandbach | How do you rate your performance in respect of the objectives noted below?
“We want to be open and transparent about the way we do business. We want to ensure local people and groups have the opportunity to ask questions about our work.” Source: https://www.sath.nhs.uk/about-us/trust-information/questions/ |
It was acknowledged at the meeting held on 7 January 2021 that there had been times when the Trust may not have been as transparent as it could have been. The Trust had made a commitment to be more transparent in the future particularly with regard to the Ockenden Review. The various ways the public can engage with the Trust including publication of Freedom of Information (FOI) requests on the website were outlined.
The Chair confirmed that the questions on the chat would be downloaded where technology allowed with responses published on the Trust’s website before the next meeting on 11 February 2021. |
| 2021/02 | 07/01/2021 | David Sandbach | Why is the Integrated Performance Report being hidden from the public? | It had been decided by the Trust that the agenda for the meeting held on 7 January 2021 would, under the circumstances, focus on the Trust’s response to the Ockenden Report published on 10 December 2020.
For this reason it was agreed that the IPR report would be published on the website as an information pack |
Public Questions Log – 08 October 2020
Question Number |
Meeting Date |
Questioner |
Question |
Answer |
|---|---|---|---|---|
| 2020/11 | 08/10/2020 | Diane Peacock*
* This question following the July 2020 Board meeting was one of a number raised at the Community Engagement meeting in December 2021 and it was agreed that the original response had not addressed the question so these were re-considered by a number of senior staff, including
Click here Community Engagement Meetings – SaTH to see response issued December 2021 which reflected the position at that time, which was some 18 months after the original meeting |
How can it be acceptable that the Trust information system is not able to ‘derive’ data on the numbers of hospital inpatient deaths that relate to care home residents based in Shropshire and in Telford & Wrekin (STW)? | Currently the Trust does not have systems in place to produce this information. The local CCG has also confirmed, that currently they also do not have systems in place to produce this information. The CEO advised it would be useful to the Trust to be able to provide this information in the future and this will be worked on for the future. |
| 2020/12 | 08/10/2020 | Diane Peacock*
* This question following the July 2020 Board meeting was one of a number raised at the Community Engagement meeting in December 2021 and it was agreed that the original response had not addressed the question so these were re-considered by a number of senior staff, including
Click here Community Engagement Meetings – SaTH to see response issued December 2021 which reflected the position at that time, which was some 18 months after the original meeting |
Can the Board please assure the public that written questions and Trust responses for July 2020 will be published retrospectively and, in future public questions with Trust responses are reported in full? | The Trust welcomes questions from the public, as they offer a different perspective on the issues discussed and additional insights into the challenges patients, staff and communities face.
The Trust requires questions to be submitted 48 hours prior to the public meeting, so the Board of Directors have time to prepare the answers. This is important as many questions require some research. The Trust will aim to answer as many questions on the day of the Board meeting as possible. Those for which an immediate response could not be prepared will be acknowledged on the day. The Trust will post the answer to outstanding questions on the website by the next meeting (or sooner where possible). If the Trust is unable to post a response within this window, the question will be acknowledged on the website, with a timeline for response. |
| 2020/12 | 08/10/2020 | Diane Peacock*
* This question following the July 2020 Board meeting was one of a number raised at the Community Engagement meeting in December 2021 and it was agreed that the original response had not addressed the question so these were re-considered by a number of senior staff, including
Click here Community Engagement Meetings – SaTH to see response issued December 2021 which reflected the position at that time, which was some 18 months after the original meeting |
The fact that outbreaks affecting care home residents in STW have been relatively low compared to other areas means local intelligence on possible causal factors could be exceptionally informative when planning to safeguard local care home residents in the event of a future surge. Given the claim that a system-wide, multi-agency partnership approach was adopted locally to deal with the first Covid-19 outbreak, why is it that a multi-agency evidence base – to evaluate locally specific multifactorial elements impacting on care home residents – is apparently not available for public scrutiny? | Local health and social care have been integrated in the safe management of patients being discharged to all care settings (including domestic homes) during Covid-19. An integrated discharge team and hub manned by hospital, social care and community staff, has been put in place, providing an invaluable function.
Local Authorities, as regional lead agencies, supported by the CCG, commission care homes and the Shropshire Partners in Care (SPIC) coordinate activities across the sector. Unfortunately the Trust does not have access to care home plans and activity. Whilst the Trust continues to monitor patients discharged to a community health and social care setting, it does not have access to the detailed Local Authorities’ lessons learnt from the first wave of Covid- 19, and benefits to residents and staff. |
| 2020/12 | 08/10/2020 | Diane Peacock*
* This question following the July 2020 Board meeting was one of a number raised at the Community Engagement meeting in December 2021 and it was agreed that the original response had not addressed the question so these were re-considered by a number of senior staff, including
Click here Community Engagement Meetings – SaTH to see response issued December 2021 which reflected the position at that time, which was some 18 months after the original meeting |
The Trust is claiming they are unable to differentiate between those patients discharged to their own home or to a residential care home at the beginning of the Covid-19 outbreak. Why is this information not available either via Capacity Tracker or as part of the various multi agency teams overseeing these processes? | The Trust’s information systems will not enable an answer to this question and the integrated discharge team hub does not hold this information either. The Trust’s new information system, tentatively scheduled to be installed in the Autumn of 2021 will solve this problem |
| 2020/12 | 08/10/2020 | Dulcie Howell | Have the Hip Operations at Telford Hospital resumed yet | This surgical area has been prioritised although some operations have not commenced as quickly as the Trust would like. The Trust’s surgical team has been asked to investigate the individual case and a clinician will be asked to contact Ms Howell. |
Public Questions Log – 30 July 2020
Question Number |
Meeting Date |
Questioner |
Question |
Answer |
|---|---|---|---|---|
| 001/2020 | 28/05/20 | Gill George | Relating to the period 1st January 2020 to the present: How many cancer patients have had their treatment delayed during this period? Who took decisions on this? What criteria were in place to determine who would be treated and who would not? I understand a decision was also taken to withhold diagnostic information from some patients (i.e. they were not told of a newly diagnosed cancer). Their treatment was therefore also delayed. How many patients were affected? Again, who took decisions on this, and based on what criteria? Were the Medical Director, Chief Executive and Board aware of the decisions to delay diagnostic information and treatment to some cancer patients? |
An extract from the minutes of the Board of Directors’ meeting on 28/05/20. At the beginning of the pandemic (March 2020) there was a clear national steer to cancel as many inpatient, ambulatory appointments and procedures as possible, in order to protect vulnerable people and create the capacity to deal with any potential surge due to the pandemic.
Whilst SaTH maintained a number of urgent surgical procedures and a full programme of radiotherapy and chemotherapy, in responding to the pandemic, the Trust recognised there have been a number of cancer patients whose diagnostics and treatment have been delayed. The Trust is not aware of any patients where the outcome of their cancer diagnosis was deliberately withheld. If you have evidence of such information being withheld, the Trust would ask you to forward it to David Holden, Interim Director of Governance (David.holden7@nhs.net). It will be investigated and the appropriate action taken. |
| 002/2020 | 30/07/202 | Gill George | The April 2020 report (from a 2019 inspection) is quite damning. It shows a failure to improve in very many areas, and a deterioration in some.
The ‘well led’ domain continues to be rated as inadequate. The report notes that the Trust breached its CQC registration with regard to 11 regulations. These included ‘Regulation 5: Fit and Proper Persons- directors’; ‘Regulation: 17: Good Governance’ and ‘Regulation 20: Duty of Candour’. These areas are fundamental. Without strong and principled leadership, the Trust will of course struggle to provide high quality clinical care. Major weaknesses in leadership were identified by the CQC in November 2018. Many of those concerns evidently remained a year later. What were the ‘Fit and Proper Persons’ breaches in November 2018? What steps were taken to resolve these? What were the ‘Fit and Proper Persons’ breaches a year later, in November 2019? Do these breaches still exist? A lack of understanding of Duty of Candour has caused great distress in the past, not least in the Trust’s handling of avoidable deaths and harm in the maternity service. What is the evidence that the current leadership team has meaningful commitment to the Duty of Candour, including a willingness to fight for a culture of openness and transparency across the organisation? Does the current Board recognise there have been damaging failures around candour in the recent past? Public board meetings since November 2018 have failed to identify ongoing weaknesses around leadership. Why? Has the Board been unaware? Or did the Board choose to withhold concerns around leadership from the public? Is the Board confident that leaders with the skills to achieve fundamental transformation at SaTH are now in place? Assuming the answer is ‘Yes’, what is the basis for that confidence? |
At the time referred to, effective governance systems were not in place to ensure all director files were complied with the ‘fit and proper persons’ regulation. The Trust could not therefore be assured that all directors were ‘fit and proper’ to carry out their responsibility for the quality and safety of care.
The Trust has since improved governance including the review of the Fit and Proper policy. The Trust commissioned its newly appointed auditors to ensure systems and processes are up to speed and good practice is being followed and maintained. |
| 003/2020 | 30/07/20 | Gill George | Former Chief Executive
What external support has SaTH received from Virginia Mason in the last year? Has this included any input from former SaTH Chief Executive Simon Wright? |
Simon Wright has not had any input into SaTH through his Virginia Mason work. |
| 004/2020 | 30/07/20 | Gill George | Staff Survey
The 2019 staff survey showed particular weaknesses around ‘themes’ of Health and Wellbeing and Staff Engagement. What steps is the Board taking to ensure that staff feel valued, listened to and supported through a difficult period? Will the Trust seek to ensure the involvement of all staff in current and future service changes, encouraging staff to see themselves as the champions of patient care and safety, and placing staff at the heart of change? The history has perhaps been one of over-reliance on a small group of senior medical staff. |
The Trust has recognised and now focused on the issues that impact staff. These include ensuring staff feel valued, listened to and supported.
The health and wellbeing of the staff re- mains a critical priority – and never more so than during this Covid period. Actions taken include:
The Trust recognises there is more to be done and we will continue to identify staff needs and respond to them. With a new leadership team in place, the Trust has already taken steps to put staff alongside patients at the heart of service changes. As an example, the Hospital Transformation Programme has been consulting with staff groups and clinical teams across the organisation about the future configuration of services. This will continue throughout the autumn to ensure their views are fully reflected in the Outline Business Case. Staff at all levels are being consulted, including Facilities, Estates, Administration and other support services, not simply senior medical and nursing staff. A new monthly information Cascade designed to reach all staff, has been well received which includes an opportunity for staff to give feedback and ask questions which are channelled back to the senior team. |
| 005/2020 | 30/07/20 | Gill George | Maternity Dashboard
The report of the Maternity Assurance Committee notes ‘A maternity dashboard was presented to the meeting’. The maternity dashboard used to be published and in the public domain as a matter of course. It was withdrawn by SaTH at a time of mounting concern about the maternity service. I have asked for publication of the maternity dashboard to be reinstated at least twice in the past. Maternity is an area of significant public interest, and it is in the interests of transparency for SaTH to share this information. Will SaTH publish the current maternity dashboard? Will SaTH make this maternity dashboard, along with previous and future maternity dashboards, available on its website? |
The Maternity Dashboard has been un- der review for several months and re- mains under review to ensure it meets national standards and follows good practice. The Trust will be reviewing publication of the dashboard, the context of the data and the Statistical Process (SPC) charts. |
| 006/2020 | 30/07/20 | Gill George | Births Before Arrival (BBAs); MLUs
(This data will be recorded by SaTH as a matter of routine and should take a few minutes to look up). |
BBA data is not a direct reflection on closure of the MLUs. This would only be significant if the number of BBAs were specifically Midwifery led women, as it is these women who should be booked for care and birth at an MLU. |
| 007/2020 | 30/07/2020 | Gill George | Cancer follow up care
This question is asked at the request of K, a SaTH patient: I’m 35, with young children. I have a serious gynaecological cancer. My initial treatment of major surgery was successful, but I continue to need regular review appts because the consequences of recurrence could be very serious indeed. My SaTH consultant has stressed the critical importance of these reviews and of these happening on time. My last booked review would have been 8 weeks overdue – but it was then cancelled, with one day’s notice. I had to make a fuss to get another appointment arranged, earlier this month. My consultant highlighted again – not just to me but to the wider service – the importance of scheduled follow up happening on time. I am due for a vault smear in early October. I received a letter from SaTH seeking to replace my appointment for a smear with a telephone appointment! This is meaningless. Again, I have had to take the responsibility for sorting out my own care. I’m tired and unwell. Cancer has changed my life. I don’t want to have to take on the job of arranging my own care, and I think many others in my situation would be unable to do this. What’s happening? Has your system for offering follow up to cancer patients broken down in the last few months? Why? What steps will SaTH take to audit existing cancer patients to ensure that people who have not been offered appropriate care will now receive high priority appointments? |
During Covid-19, cancer services continued as a priority. All appointments were triaged by a consultant to ensure that an appropriate appointment option was offered. Where appropriate, telephone follow ups were offered rather than face to face, and some follow up appointments were converted into telephone or consultations via other means.
It would not be usual for a smear appointment to be replaced with a telephone call, but this may have been a result of consultant triage as above. Waiting time targets continue to be achieved in gynaecology, and all patients on a follow up list are reviewed. |
| 008/2020 | 30/07/2020 | Claire Howard, Parkinsons UK | Parkinson’s Nurse Specialist (PNS) post
In December 2019, following a number of conversations and meetings over the previous eighteen months, SaTH’s Chief Operating Officer and Assistant Chief Operating Officer informed Parkinson’s UK that the Trust had committed to recruiting to the vacant Parkinson’s Nurse Specialist (PNS) post. However this post is still vacant and has not been advertised. Parkinson’s UK understands the constrictions Covid placed on trusts’ capacity for recruitment but we are also keenly aware that, for more than two years, people with Parkinson’s have had limited access to a specialist nurse service in Shropshire. We are also aware that a number of other trusts have success- fully recruited to these posts in recent months. Please can the board advise when the post will be advertised?” If there are any problems with this then please let me know. 29/07/20 It’s great to hear that there is a plan to recruit and would be grateful to be kept updated on this process. I would also just like to confirm that this question will still be presented to and answered by the board this afternoon so that there is public acknowledgement of this? I hope that this would also then provide some reassurance to the Parkinson’s community in Shropshire. |
SaTH has a Parkinson’s Specialist Nurse in post based at PRH in Neurology Services and is in the process of recruiting a second one. |
| 009/2020 | 30/07/2020 | Diane Peacock*
* This question following the July 2020 Board meeting was one of a number raised at the Community Engagement meeting in December 2021 and it was agreed that the original response had not addressed the question so these were re-considered by a number of senior staff, including
Click here Community Engagement Meetings – SaTH to see response issued December 2021 which reflected the position at that time, which was some 18 months after the original meeting |
Various Questions
The questions below are intended to provide the public with information relating to the local outcomes of national directives and guidance on hospital admissions and discharges, from and into care homes in Shropshire and in Telford & Wrekin during Covid-19. In the interest of accessibility and transparency, the Governing Body is politely requested to supply actual numbers and dates when responding to questions 1-5.
|
|
| 010/2020 | 30/07/20 | David Sandbach | Various Questions
Replacement wording ‘Prof Deadman (NED) high- lighted that the same serious WLI implementation policy issues appear to have been identified and reportedly resolved by successive audit committee re- views in the last 9 years. We therefore need to check that when WLI audit actions are reported as completed they result in lasting improvements. Yet another example of bad management at SaTH this comment looks like others whereby NED’s complain about management inability to make plans stick on a permanent basis. See also – “Mr Allen (A.NED) made the point with regard to action plans that the Trust is good at finding solutions but these are not sustainable.” What does “embedded” mean?
“the Trust’s Maternity Assurance Committee is also adding performance assurance rigour into the Care Group” In February this year I pointed out this facility:
Source: MBRACE Perinatal Mortality Surveillance Report page 38. Given the real time nature of this reporting system I would expect the Executive led Maternity Quality Committee and the MAC would find it a very rigorous assurance measurement tool. “Prof Deadman (NED) stated that he was pleased to note that the Trust has implemented an outpatient virtual consultation solution as part of the response to Covid-19.” SEE: https://www.sath.nhs.uk/patients-visitors/video-clinics/ Why have some of the surgical specialties e.g. vascular and colorectal not signed up to offering virtual clinics? Has an evaluation methodology / evaluation team been established? “Mr Newman asked if the Trust has a date by which it will be back on plan for cancer performance and diagnostics. He noted that the IPR is reporting the historical position, and provides no evidence of service recovery proposals. The COO responded that as part of the immediate restoration work the Trust has introduced some urgent services, and that extensive discussion is currently underway on how restoration is further developed as part of the Operational Plan.” May 28th 2020 Board members may like to see this report from the SCCG Board papers dated 8th July 2020 to get a feel for the situation in the Shropshire CCG area:
https://www.shropshireccg.nhs.uk/media/2818/08072020-combined-part-1-sccg-governing-body-papers.pdf MONTHLY INTEGRATED PERFORMANCE REPORT The Board of Directors noted the report, and the Chair requested that future reports incorporate a more forward looking focus. Need to check this is in the Board papers. “The committee received a high level Draft Maternity Transformation Plan to bring the maternity services to where we need to be in the future. This is largely based on themes identified from the leaked DO re- port and aligns to Morecombe Bay report.” Should the people of Shropshire, especially women of childbearing age, raise a glass of campaign to whoever leaked the DO report? Emergency Department Assurance Committee Key Issues Report The fundamental risk to Emergency Department performance is the mad cap, NHS establishment denial of reality by the SaTH Board, CCG’s and NHSE/I. (Recovery Plan included on agenda for discussion at Finance & Performance (August 2020). Unless and until there is a centralised A&E department along the lines of the FF plan SaTH performance will remain abysmal for the next 5 – 6 years. These words will appear in the audit reports year on year: “KPMG was not satisfied that the Trust made proper arrangements to secure economy, efficiency and effectiveness in its use of resources. This was due to its financial position, high agency spend, inadequate CQC rating, failure to deliver a number of operational targets and the independent review into maternity care.” I truly wish the SaTH Board did not believe that the earth is flat and that fundamental forces of clinical demand spread over two half-baked departments cannot be managed by re-arranging the corporate policy furniture and so called “help” from people who do not have any real skin in this game. The backlog of patients waiting for Diagnostics and Treatment has risen significantly during Q1 and additional capacity will be required to address this during the remainder of 2020/21”. No Board paper explaining what the plan is to deal with the issue. A winter pressure plan is promised for the Board in September a few weeks before winter starts in the NHS. “We are planning carefully for the months ahead including winter.” CEO report NEDs need more detail – as do the public. This comment is not good enough at this point in the winter planning cycle: I refer you to my plan to open a Covid safe facility in Telford – at least it is a plan. NEDs should open these links and ask if SaTH has plans to introduce this technology “Call before you Attend service.” https://www.england.nhs.uk/wp-content/uploads/2020/07/Agenda-item-5-Future-of-UEC-services.pdf and this https://www.theguardian.com/society/2019/may/23/birmingham-to-begin-accident-and- emergency-online-chat-service-in-tech-revolution-for-nhs-care SATH UTC Activity and care at the MIUs continues to provide patients with a beneficial alternative to ED” This is not what the SCCG is saying in their Board papers.
Is this performance because SaTH is short of MRI’s and CT scanners? |
The Trust has reviewed these audits and found no evidence of fraud. The Trust has reviewed job plans with individual consultants and identified explanations for audit findings relating to job planning and flexible working. It has provided clearer guidance for doctors. The Trust has amended relevant policies and introduced improved more accountable processes.
In the CQC improvement plan, embedded means, sufficient time has been allowed to ensure systems, process and change have occurred to ensure the action is completed. For example: Following the development of a new pol- icy, embedding would mean actions are applied consistently with tangible and measurable benefits for patient out- comes. Cancer forecast included in Operational Plan (slide 5 & 6). Detail included in August IPR will be presented at Board of Directors Meeting on 17.09.20. Recovery Plan included on agenda for discussion at Finance & Performance (August 2020). The Trust is exploring the “Think 111 first” model and has requested data from other Trusts using it. Recognising the availability of other options, the Trust is being mindful not to increase ED attendances and is working with partners to expand the urgent treatment centre models. The activity taking place at MIUs continues to allow some patients to access care at the 2 MIU sites rather than attend the 2 Emergency departments – this reduces risk for staff and patients. The graph (attached) relates to the national diagnostic standard (DM01) – the aim is for 99% of planned diagnostic tests to take place within 6 weeks of the referral. The standard includes not only CT/MRI/Ultrasound, but also Endoscopy and Physiological Measurements such as ECGs and Audiology. In May, in line with national guidance, routine diagnostics were paused. SaTH was, and still is, unable to carry out the same number of tests per hour as pre-Covid. Referrals to all diagnostic modalities are prioritised based on clinical urgency. Pre Covid, SATH had one of the highest usage rates per scanner for CT and MRI in the region, and reductions in throughput due to social distancing and infection control measures does mean that the Trust requires more scanner capacity. In July, August and September, NHSI have supported SATH with mobile CT, and in October we will have both mobile CT and mobile MRI capacity to support increased imaging. |